Você também pode gostar
- Troubled Bodies: Critical Perspectives on Postmodernism, Medical Ethics, and the BodyNo EverandTroubled Bodies: Critical Perspectives on Postmodernism, Medical Ethics, and the BodyAinda não há avaliações
- Technocratic Humanistic and HolisticDocumento21 páginasTechnocratic Humanistic and HolisticritablAinda não há avaliações
- Resilient Cyborgs: Living and Dying with Pacemakers and DefibrillatorsNo EverandResilient Cyborgs: Living and Dying with Pacemakers and DefibrillatorsAinda não há avaliações
- Intuition As Authoritative Knowledge in Midwifery and HomebirthDocumento34 páginasIntuition As Authoritative Knowledge in Midwifery and HomebirthVanesa Gi - GaAinda não há avaliações
- Experiments in Love and Death: Medicine, Postmodernism, Microethics and the BodyNo EverandExperiments in Love and Death: Medicine, Postmodernism, Microethics and the BodyAinda não há avaliações
- LESLIE Charles - Medical PluralismDocumento5 páginasLESLIE Charles - Medical PluralismJocelynLeyvaAinda não há avaliações
- Biotechnology and Culture: Bodies, Anxieties, EthicsNo EverandBiotechnology and Culture: Bodies, Anxieties, EthicsPaul E. BrodwinAinda não há avaliações
- Research Paper Medical AnthropologyDocumento7 páginasResearch Paper Medical Anthropologymwjhkmrif100% (1)
- Limits to Medicine: Medical Nemesis: The Expropriation of HealthNo EverandLimits to Medicine: Medical Nemesis: The Expropriation of HealthAinda não há avaliações
- (Philosophy and Medicine 43) Drew Leder (Auth.), Drew Leder (Eds.) - The Body in Medical Thought and Practice-Springer Netherlands (1992) PDFDocumento255 páginas(Philosophy and Medicine 43) Drew Leder (Auth.), Drew Leder (Eds.) - The Body in Medical Thought and Practice-Springer Netherlands (1992) PDFAlejandro LareginaAinda não há avaliações
- Covenantal Biomedical Ethics for Contemporary Medicine: An Alternative to Principles-Based EthicsNo EverandCovenantal Biomedical Ethics for Contemporary Medicine: An Alternative to Principles-Based EthicsAinda não há avaliações
- Cross-Cultural Medicine: Multi Causality: Consequences For Medical PracticeDocumento7 páginasCross-Cultural Medicine: Multi Causality: Consequences For Medical PracticeDikara Widyangga Sulfian MaulidyAinda não há avaliações
- Human Life Its Philosophy and Laws: An Exposition of the Principles and Practices of OrthopathyNo EverandHuman Life Its Philosophy and Laws: An Exposition of the Principles and Practices of OrthopathyAinda não há avaliações
- Bleakley (2014) - Patient-Centred Medicine in TransitionDocumento271 páginasBleakley (2014) - Patient-Centred Medicine in TransitionFrancoLacuesta100% (1)
- The Principles of Occult Healing - A Working Hypothesis Which Includes All Cures - Studies by a Group of Theosophical StudentsNo EverandThe Principles of Occult Healing - A Working Hypothesis Which Includes All Cures - Studies by a Group of Theosophical StudentsNota: 3 de 5 estrelas3/5 (2)
- The Virus Misconception, Part III (Mobile Version)Documento22 páginasThe Virus Misconception, Part III (Mobile Version)Franco CognitiAinda não há avaliações
- Narrative Medicine in Education, Practice, and InterventionsNo EverandNarrative Medicine in Education, Practice, and InterventionsAinda não há avaliações
- CLARIFYING THE DISCIPLINE OF NURSING AS FOUNDATIONAL - J Watson - 2017Documento2 páginasCLARIFYING THE DISCIPLINE OF NURSING AS FOUNDATIONAL - J Watson - 2017Nuno FerreiraAinda não há avaliações
- Jmedeth00154 0024Documento5 páginasJmedeth00154 0024Valentina De SoldaAinda não há avaliações
- Journal of Medical Ethics and History of Medicine: Is Dissection Humane?Documento4 páginasJournal of Medical Ethics and History of Medicine: Is Dissection Humane?Rahmat SatriadiAinda não há avaliações
- Lock BiotechnologiesDocumento6 páginasLock BiotechnologiesLëteme ViAinda não há avaliações
- SHILDRICK Corporeal Cuts Surgery and TheDocumento16 páginasSHILDRICK Corporeal Cuts Surgery and TheMadalina ElenaAinda não há avaliações
- Ivan Ilyich - Limits-To-Medicine 1976 (Spanish)Documento7 páginasIvan Ilyich - Limits-To-Medicine 1976 (Spanish)timstr777Ainda não há avaliações
- Reinscribing The Birthing Body:: Homebirth As Ritual PerformanceDocumento24 páginasReinscribing The Birthing Body:: Homebirth As Ritual PerformanceAnaAinda não há avaliações
- Social Ethics in Technocratic EraDocumento14 páginasSocial Ethics in Technocratic EraNoel JonasAinda não há avaliações
- Krieger Nancy Epidemiology and The PeopleDocumento394 páginasKrieger Nancy Epidemiology and The PeopleAnamaria Zaccolo100% (1)
- Krieger Nancy Epidemiology and The People-1-297Documento297 páginasKrieger Nancy Epidemiology and The People-1-297Luiza MenezesAinda não há avaliações
- The Virtuous Physician The Role of Virtue in Medicine (Philosophy and Medicine, Vol. 114) 2012th Edition (PRG)Documento256 páginasThe Virtuous Physician The Role of Virtue in Medicine (Philosophy and Medicine, Vol. 114) 2012th Edition (PRG)hanalaras100% (2)
- Bio Mechanical and Phenomenological Models of The Body, The Meaning of IllnessDocumento10 páginasBio Mechanical and Phenomenological Models of The Body, The Meaning of IllnessHusserlAinda não há avaliações
- Session - 4 - Sociology - of - Social - Control - Study - GuideDocumento4 páginasSession - 4 - Sociology - of - Social - Control - Study - GuideSammyAinda não há avaliações
- S. Lanka - The-Virus-Misconception-Part 3Documento8 páginasS. Lanka - The-Virus-Misconception-Part 3Kimi SikitaAinda não há avaliações
- The Technocratic Body: American Childbirth As Cultural ExpressionDocumento16 páginasThe Technocratic Body: American Childbirth As Cultural ExpressionArthur ZanchetAinda não há avaliações
- Progenitors (Convention: Mage The Ascension)Documento7 páginasProgenitors (Convention: Mage The Ascension)Beth100% (2)
- Canguilhem The New NormalDocumento11 páginasCanguilhem The New NormalFahmi Ben HfaiedhAinda não há avaliações
- Causal Layered Analysis Defined: by Sohail InayatullahDocumento1 páginaCausal Layered Analysis Defined: by Sohail InayatullahAmi ZenAinda não há avaliações
- Kinghorn Et Al, Does The Emperor Have Any ClothesDocumento6 páginasKinghorn Et Al, Does The Emperor Have Any ClothesBob DoleAinda não há avaliações
- Wissenschafftplus VirologistsDocumento11 páginasWissenschafftplus VirologistsJoan DzimwashaAinda não há avaliações
- Care in Practice MOL PDFDocumento14 páginasCare in Practice MOL PDFPedroFragosoAinda não há avaliações
- The Impact of Arab Culture On Psychiatric Ethics - Ahmed OkashaDocumento14 páginasThe Impact of Arab Culture On Psychiatric Ethics - Ahmed OkashamoftasaAinda não há avaliações
- Cahill 2000 PDFDocumento9 páginasCahill 2000 PDFAnnah CholletAinda não há avaliações
- MEDICAL PROFESSION AS A MORAL COMMUNITY - E D Pellegrino - Bullnyacadmed00014-0025Documento12 páginasMEDICAL PROFESSION AS A MORAL COMMUNITY - E D Pellegrino - Bullnyacadmed00014-0025Bayu PramanaAinda não há avaliações
- El Parto y El Nacimiento en La ModernidadDocumento11 páginasEl Parto y El Nacimiento en La ModernidadYohani LopezAinda não há avaliações
- A Nursing TheoryDocumento3 páginasA Nursing TheoryVanessa GonzalezAinda não há avaliações
- The Tecnocratic Model of Birth-Robbie Davis-FloydDocumento17 páginasThe Tecnocratic Model of Birth-Robbie Davis-FloydDalia MoraAinda não há avaliações
- Global Perspectives On Stem Cell Technologies 1St Edition Aditya Bharadwaj Eds Full ChapterDocumento67 páginasGlobal Perspectives On Stem Cell Technologies 1St Edition Aditya Bharadwaj Eds Full Chapterdiana.smith975100% (5)
- Unified Concept of Health and DiseaseDocumento28 páginasUnified Concept of Health and DiseaseHossam BarghashAinda não há avaliações
- Homo Economicus and Life Markets Biehl 2011 Medical Anthropology QuarterlyDocumento7 páginasHomo Economicus and Life Markets Biehl 2011 Medical Anthropology QuarterlyAvimar JuniorAinda não há avaliações
- Banking Time' - Egg Freezing and The Negotiation of Future FertilityDocumento14 páginasBanking Time' - Egg Freezing and The Negotiation of Future FertilityPaula Manalo-SuliguinAinda não há avaliações
- De GruyterDocumento17 páginasDe Gruyterisabella granataAinda não há avaliações
- Editorial FromtheorytopracticeDocumento5 páginasEditorial FromtheorytopracticeAditya WaghAinda não há avaliações
- Papadimos, T. J. (2004) - Stoicism, The Physician, and Care of Medical Outliers.Documento7 páginasPapadimos, T. J. (2004) - Stoicism, The Physician, and Care of Medical Outliers.Prof.V. GunaretnamAinda não há avaliações
- MacKenzie - What Would A Good Doctor Do? Re Ections On The Ethics of MedicineDocumento4 páginasMacKenzie - What Would A Good Doctor Do? Re Ections On The Ethics of MedicineCecitorAinda não há avaliações
- El Modelo de Salutogénesis InglésDocumento8 páginasEl Modelo de Salutogénesis InglésMiguel Angel Alemany NaveirasAinda não há avaliações
- The Technocratic Model of BirthDocumento18 páginasThe Technocratic Model of BirthA. J. BeyAinda não há avaliações
- Stoicism, The Physician, and Care of Medical Outliers: BMC Medical Ethics January 2005Documento8 páginasStoicism, The Physician, and Care of Medical Outliers: BMC Medical Ethics January 2005mroctavAinda não há avaliações
- The Clinical Application of The Biopsychosocial ModelDocumento24 páginasThe Clinical Application of The Biopsychosocial ModelLuis Alberto González SalomónAinda não há avaliações
- Body & Society: Corporeal Cuts: Surgery and The Psycho-SocialDocumento17 páginasBody & Society: Corporeal Cuts: Surgery and The Psycho-Socialmarta vilarinhoAinda não há avaliações
- Final Project 4 RewriteDocumento11 páginasFinal Project 4 Rewriteapi-710396108Ainda não há avaliações
- Bioethics: Contra Gentiles of St. Thomas Aquinas (1224/25-1274), Which Briefly Discusses TheDocumento7 páginasBioethics: Contra Gentiles of St. Thomas Aquinas (1224/25-1274), Which Briefly Discusses TheBusk 93Ainda não há avaliações
- KRANNER, Catalina y RADOSTA, Darío - Parto Respetado y Buena MuerteDocumento24 páginasKRANNER, Catalina y RADOSTA, Darío - Parto Respetado y Buena MuerteAgus ZanettiAinda não há avaliações
- WDG 4Documento2 páginasWDG 4Anonymous rNLEUdAinda não há avaliações
- sm-g361h DsDocumento44 páginassm-g361h DsTest TestAinda não há avaliações
- Denon Avr-1613 Owners ManualDocumento131 páginasDenon Avr-1613 Owners ManuallerondotAinda não há avaliações
- Energy Efficient BuildingDocumento11 páginasEnergy Efficient BuildingSantosh Basnet100% (2)
- Connecting To The Internet With Pico WDocumento30 páginasConnecting To The Internet With Pico WKnut BoergeAinda não há avaliações
- 15kw - SN College - SLDDocumento1 página15kw - SN College - SLDmebin k XavierAinda não há avaliações
- FPR de Weck Jul 1 2012Documento59 páginasFPR de Weck Jul 1 2012rmAinda não há avaliações
- Get More From Your: MIRO Power Quality Logger and Analyser Starter KitsDocumento5 páginasGet More From Your: MIRO Power Quality Logger and Analyser Starter Kitsjobpei2Ainda não há avaliações
- Pe 001Documento216 páginasPe 001erivan bernardoAinda não há avaliações
- Integrating Microsoft Access With Autocad VbaDocumento19 páginasIntegrating Microsoft Access With Autocad VbaLuiz Paulo Cruz JrAinda não há avaliações
- AOC LCD MonitorDocumento60 páginasAOC LCD MonitorRoger Martínez BermúdezAinda não há avaliações
- Level 50 - How Can CSP Partners Build A Business With AzureDocumento56 páginasLevel 50 - How Can CSP Partners Build A Business With Azureaki koshaAinda não há avaliações
- DTN NS3Documento4 páginasDTN NS3Mirza RizkyAinda não há avaliações
- General Notes: Fourth Floor PlanDocumento1 páginaGeneral Notes: Fourth Floor PlanJuan IstilAinda não há avaliações
- Wilmont's DroneTech Project Charter PDFDocumento2 páginasWilmont's DroneTech Project Charter PDFhuda mahmoudAinda não há avaliações
- Bova Futura Electrical System ManualDocumento40 páginasBova Futura Electrical System ManualmagzigioAinda não há avaliações
- ENG DS OSA Series Relay Data Sheet E 0411Documento3 páginasENG DS OSA Series Relay Data Sheet E 0411Klisman Rafael Santi RamosAinda não há avaliações
- CV Iqbal 2016Documento3 páginasCV Iqbal 2016Muhammad Iqbal ImaduddinAinda não há avaliações
- AWS Academy Cloud Foundations Module 05 Student GuideDocumento75 páginasAWS Academy Cloud Foundations Module 05 Student GuidevalzAinda não há avaliações
- Prime Time FeaturesDocumento15 páginasPrime Time FeaturesPruthwish PatelAinda não há avaliações
- SAP - ABAP CDS Development User Guide: WarningDocumento91 páginasSAP - ABAP CDS Development User Guide: WarningKrishna Kshera SagareAinda não há avaliações
- Parking Example - JAVADocumento4 páginasParking Example - JAVAMuhammad Rana Farhan100% (1)
- Genset Canopy DesignDocumento10 páginasGenset Canopy DesignNick JohnsonnAinda não há avaliações
- Pert ChartDocumento20 páginasPert Chartshweta bhilawadiAinda não há avaliações
- House Wiring ReportDocumento9 páginasHouse Wiring ReportCovid VirusAinda não há avaliações
- Application For Getting ISBN Number in IndiaDocumento3 páginasApplication For Getting ISBN Number in IndiamahamayaAinda não há avaliações
- Biomedical 7-8Documento20 páginasBiomedical 7-8முத்துலிங்கம். பால்ராஜ்Ainda não há avaliações
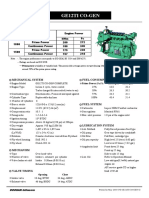
- Ge12ti Co Gen-GDocumento2 páginasGe12ti Co Gen-GTilok DasAinda não há avaliações
- Pbdocs Traktoren Zetor 117 41 Forterra eDocumento1 páginaPbdocs Traktoren Zetor 117 41 Forterra eZoran RajčevićAinda não há avaliações
- ScriptCase 9.6.018 Crack Serial Number Latest Keygen Download 2021Documento1 páginaScriptCase 9.6.018 Crack Serial Number Latest Keygen Download 2021DILANE PRO officielAinda não há avaliações
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nota: 3 de 5 estrelas3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 4.5 de 5 estrelas4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (32)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 4 de 5 estrelas4/5 (4)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNo EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisNota: 3.5 de 5 estrelas3.5/5 (2)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (170)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNo EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNota: 4.5 de 5 estrelas4.5/5 (1412)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceNo EverandTo Explain the World: The Discovery of Modern ScienceNota: 3.5 de 5 estrelas3.5/5 (51)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNo EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNota: 4 de 5 estrelas4/5 (46)
- The Marshmallow Test: Mastering Self-ControlNo EverandThe Marshmallow Test: Mastering Self-ControlNota: 4.5 de 5 estrelas4.5/5 (60)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (328)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4.5 de 5 estrelas4.5/5 (6)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNo EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNota: 1 de 5 estrelas1/5 (1)