Você também pode gostar
- Culture - WikipediaDocumento94 páginasCulture - WikipediaKranthi Austin's100% (1)
- Health & Safety AssignmentDocumento15 páginasHealth & Safety AssignmentRetish DeshmukhAinda não há avaliações
- Chemical Management D0cc1a52 2a03 4d29 Ac14 E8c1544c1c82Documento4 páginasChemical Management D0cc1a52 2a03 4d29 Ac14 E8c1544c1c82Arslan Haider100% (1)
- Igcse Geography 1. Population DynamicsDocumento48 páginasIgcse Geography 1. Population DynamicsAyoub Ibn AhmedAinda não há avaliações
- Vehicles Techniques Extrication GB WebDocumento95 páginasVehicles Techniques Extrication GB WebFrancisco BorgesAinda não há avaliações
- Population Dynamics: Bio 1 Hon: Chapter 4 Section 1 Bio 1: Chapter 14 Sections 3 and 4Documento10 páginasPopulation Dynamics: Bio 1 Hon: Chapter 4 Section 1 Bio 1: Chapter 14 Sections 3 and 4Sonya Naser KhellaAinda não há avaliações
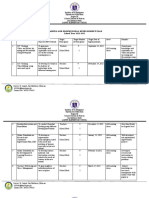
- Lapnit ES - Training and Professional Development PlanDocumento4 páginasLapnit ES - Training and Professional Development PlanJessa VillanuevaAinda não há avaliações
- Oh S Management SystemDocumento25 páginasOh S Management Systempaulina15vAinda não há avaliações
- Vehicle Final Inspection Checklist FormDocumento5 páginasVehicle Final Inspection Checklist FormLaurelle RaynersAinda não há avaliações
- SMK Sentosa Yearly Lesson Plan 2019 Mathematics Form 2Documento17 páginasSMK Sentosa Yearly Lesson Plan 2019 Mathematics Form 2IffahJusohAinda não há avaliações
- First Aid KitDocumento24 páginasFirst Aid KitCaleb ConnerAinda não há avaliações
- Topic 4 Osh PolipdDocumento55 páginasTopic 4 Osh PolipdHarish Nagoor NahooranAinda não há avaliações
- CP - 109 - Safe Work Obsevation ProcessDocumento8 páginasCP - 109 - Safe Work Obsevation ProcessYusufAinda não há avaliações
- Hirarc SharpDocumento29 páginasHirarc Sharpczhong16Ainda não há avaliações
- Anatomy and Physiology of The Circulatory and Vascular SystemsDocumento25 páginasAnatomy and Physiology of The Circulatory and Vascular SystemsPrince Rener Velasco PeraAinda não há avaliações
- Osha Individual ReportDocumento36 páginasOsha Individual ReportIz'aan Syafiq RoslanAinda não há avaliações
- DMSG-13-30 HSE Risk Assessment: DNV GL Management SystemDocumento3 páginasDMSG-13-30 HSE Risk Assessment: DNV GL Management SystemWilliam VazquezAinda não há avaliações
- Musculosleketal Risk Assesment Among Nurses in Pateint Manual Handling in Hospital Wards - A Cross Sectional StudyDocumento10 páginasMusculosleketal Risk Assesment Among Nurses in Pateint Manual Handling in Hospital Wards - A Cross Sectional StudyCureusAinda não há avaliações
- Ergonomics: Pallavi WakodeDocumento49 páginasErgonomics: Pallavi WakodeAkshay BangadAinda não há avaliações
- CM - Community Diagnosis - ParasDocumento83 páginasCM - Community Diagnosis - ParasHoque Mohammed Newaz Shoriful100% (1)
- Lecture 1 Introduction To Industrial HygieneDocumento40 páginasLecture 1 Introduction To Industrial Hygienesiti zubaidahAinda não há avaliações
- Mental HealthDocumento4 páginasMental HealthAhmad Ade aqomuddinAinda não há avaliações
- Procedures - Sharps Management and Injury ProtocolDocumento6 páginasProcedures - Sharps Management and Injury ProtocolMarwan GamaleldinAinda não há avaliações
- Click On The Grey Button Beside The Correct Answer: Bloodborne Pathogen QuizDocumento5 páginasClick On The Grey Button Beside The Correct Answer: Bloodborne Pathogen Quizjhun1203Ainda não há avaliações
- National Association of Safety ProfessionalsDocumento78 páginasNational Association of Safety Professionalsapi-19846338100% (1)
- 2.1. Organising For SafetyDocumento29 páginas2.1. Organising For SafetyPERATCHI SELVANAinda não há avaliações
- Infectious Disease Management One Health CourseDocumento177 páginasInfectious Disease Management One Health CourseNisa AzzaleaAinda não há avaliações
- Spillage ProcedureDocumento5 páginasSpillage ProcedureSamatha BiotechAinda não há avaliações
- Quiz Worksheet Autonomy in Psychosocial Growth PDFDocumento1 páginaQuiz Worksheet Autonomy in Psychosocial Growth PDFAndrei PostolacheAinda não há avaliações
- Hazard Identification, Risk Assessment and Risk Control (HIRARC)Documento8 páginasHazard Identification, Risk Assessment and Risk Control (HIRARC)Farah AtiqahAinda não há avaliações
- Earthquake Drill Observation ChecklistDocumento2 páginasEarthquake Drill Observation ChecklistSunny Jr DemandanteAinda não há avaliações
- All Accident Are IncidentDocumento6 páginasAll Accident Are IncidenttemterAinda não há avaliações
- Lecture#1 Introduction To Lab SafetyDocumento24 páginasLecture#1 Introduction To Lab SafetyFatima AlkhusaibiAinda não há avaliações
- Project HSE Measurement PlanDocumento2 páginasProject HSE Measurement PlanBishop Ojonuguwa AmehAinda não há avaliações
- Training On ISO 45001 - CopieDocumento47 páginasTraining On ISO 45001 - Copiekoum junior100% (1)
- Reproductive System NotesDocumento36 páginasReproductive System Notesapi-263915931100% (1)
- Nursing Division BudgetingDocumento5 páginasNursing Division BudgetingGeorgeEchevarriaAinda não há avaliações
- Safety GoalsDocumento18 páginasSafety Goalsprisma1Ainda não há avaliações
- Do 208 MH Workplace GuidelinesDocumento42 páginasDo 208 MH Workplace GuidelinesxavAinda não há avaliações
- Spillage Management: Arrangements AND GuidanceDocumento10 páginasSpillage Management: Arrangements AND GuidanceSamatha BiotechAinda não há avaliações
- Health and Safety ScopeDocumento12 páginasHealth and Safety ScopeMuhammad Shahood JamalAinda não há avaliações
- Opening and Operating A Retail BakeryDocumento322 páginasOpening and Operating A Retail BakerySantiago MathiasenAinda não há avaliações
- Recovery High Schools in Massachusetts: A Promising, Comprehensive Model For Adolescent Substance Abuse and DependenceDocumento44 páginasRecovery High Schools in Massachusetts: A Promising, Comprehensive Model For Adolescent Substance Abuse and DependenceThe Stacie Mathewson FoundationAinda não há avaliações
- Occupational Health Hazards and Workers' Health: Marissa G. Lomuntad - San Jose, MD, MOHDocumento86 páginasOccupational Health Hazards and Workers' Health: Marissa G. Lomuntad - San Jose, MD, MOHAviects Avie JaroAinda não há avaliações
- Chemical Safety ReportDocumento8 páginasChemical Safety Reporteeb1666Ainda não há avaliações
- Neurobiologic Theories and PsychopharmacologyDocumento2 páginasNeurobiologic Theories and Psychopharmacologymyer pasandalanAinda não há avaliações
- Safety Orientation - Warehouse OperationsDocumento66 páginasSafety Orientation - Warehouse OperationsRalph CastilloAinda não há avaliações
- Best Practices Physical Hazard ControlDocumento224 páginasBest Practices Physical Hazard ControlFarah farahAinda não há avaliações
- Manual Work HandlingDocumento8 páginasManual Work HandlingjoshivishwanathAinda não há avaliações
- 13 Needle-Stick InjuriesDocumento9 páginas13 Needle-Stick InjuriesveraAinda não há avaliações
- Periodic Health ExaminationDocumento38 páginasPeriodic Health ExaminationHilma NadhifaAinda não há avaliações
- Oral Glucose Tolerance TestDocumento4 páginasOral Glucose Tolerance TestCyna Jane Yao AlcularAinda não há avaliações
- Provision of A Safe EnvironmentDocumento19 páginasProvision of A Safe EnvironmentKristian Jane de JesusAinda não há avaliações
- Ecs258 - Lab Report (Co4: Po4) : Faculty of Civil EngineeringDocumento2 páginasEcs258 - Lab Report (Co4: Po4) : Faculty of Civil EngineeringAbdullah AsyraffAinda não há avaliações
- System Safety Rules - v4.1Documento116 páginasSystem Safety Rules - v4.1salman KhanAinda não há avaliações
- G5 Science Week 11Documento30 páginasG5 Science Week 11Park Vincent PrinceAinda não há avaliações
- Waste ManagementDocumento21 páginasWaste ManagementBeta UserAinda não há avaliações
- HealthfacilityplanDocumento18 páginasHealthfacilityplanapi-228206146Ainda não há avaliações
- Mass Casualty Disaster Plan Checklist: A Template For Healthcare FacilitiesDocumento18 páginasMass Casualty Disaster Plan Checklist: A Template For Healthcare FacilitiesRamon Billy0% (1)
- Contengincy Plan PortfolioDocumento5 páginasContengincy Plan Portfolioapi-397923551Ainda não há avaliações
- Class PlanDocumento5 páginasClass PlanSagrina BangunAinda não há avaliações
- (Desa / Dusun) : A. WashDocumento5 páginas(Desa / Dusun) : A. WashSagrina BangunAinda não há avaliações
- Safe HospitalDocumento36 páginasSafe HospitalSagrina BangunAinda não há avaliações
- Kajian Resiko Bencana Tanah LongsorDocumento11 páginasKajian Resiko Bencana Tanah LongsorSagrina BangunAinda não há avaliações
- Case Study - Higher Education: CommunityDocumento6 páginasCase Study - Higher Education: CommunitySagrina BangunAinda não há avaliações
- PRC-Logframe Granite Project SosekDocumento5 páginasPRC-Logframe Granite Project SosekSagrina BangunAinda não há avaliações
- Logframe WFPDocumento8 páginasLogframe WFPSagrina BangunAinda não há avaliações
- All The Love in The World LyricsDocumento1 páginaAll The Love in The World LyricsSagrina BangunAinda não há avaliações
- IB Final ShellDocumento25 páginasIB Final ShellsnehakopadeAinda não há avaliações
- Damghan EarthquakeDocumento4 páginasDamghan EarthquakeriyaAinda não há avaliações
- Genres of Text EditedDocumento5 páginasGenres of Text EditedElvira EkaAinda não há avaliações
- Voices From Chernobyl-Text For PerformanceDocumento22 páginasVoices From Chernobyl-Text For PerformanceFairewinds Energy Education100% (1)
- What Is A Force Majeure Contract Clause, and How Does It Work?Documento8 páginasWhat Is A Force Majeure Contract Clause, and How Does It Work?SubbuAinda não há avaliações
- Emergency Preparedness & Response ProcedureDocumento6 páginasEmergency Preparedness & Response ProcedureRo Selle100% (2)
- Draft: The Revised Minimum Standards For The National Service Training Program ModulesDocumento16 páginasDraft: The Revised Minimum Standards For The National Service Training Program Modulesraul gironella100% (1)
- Tropical Cyclones: Group 2 MembersDocumento7 páginasTropical Cyclones: Group 2 MembersJusty CadungogAinda não há avaliações
- Seismic Load CalculationDocumento6 páginasSeismic Load Calculationjoshua humirangAinda não há avaliações
- 2 09P01 PDFDocumento54 páginas2 09P01 PDFMike2322Ainda não há avaliações
- Second Quarter-Module 5 Week 5 Second Quarter - Module 5: First Qsecondodule 5Documento12 páginasSecond Quarter-Module 5 Week 5 Second Quarter - Module 5: First Qsecondodule 5Michael Angelo ValdezAinda não há avaliações
- Real Smolensk Executive Summary of The Technical ReportDocumento3 páginasReal Smolensk Executive Summary of The Technical Reportamadar1Ainda não há avaliações
- Composition A 5Documento3 páginasComposition A 5Frank Der-BesteAinda não há avaliações
- Division of Zamboanga Sibugay: Earthquake Drill Evaluation FormDocumento1 páginaDivision of Zamboanga Sibugay: Earthquake Drill Evaluation FormSachi SummersAinda não há avaliações
- BBC Peoples War Royal NavyDocumento342 páginasBBC Peoples War Royal NavyGraham MooreAinda não há avaliações
- Luyện BT theo chuyên đề - 2022 AutosavedDocumento25 páginasLuyện BT theo chuyên đề - 2022 Autosaved04.Nguyễn Hà Quỳnh AnhAinda não há avaliações
- 4th MagazineDocumento116 páginas4th MagazineMike Medina100% (1)
- Quotation Asuransi SPBE PT. Pelita GrahaDocumento4 páginasQuotation Asuransi SPBE PT. Pelita GrahaAgung SaputroAinda não há avaliações
- Challenger Space Shuttle DisasterDocumento2 páginasChallenger Space Shuttle DisasterPiyush ChauhanAinda não há avaliações
- Mount Everest Discussion Questions-1Documento1 páginaMount Everest Discussion Questions-1Foram NaikAinda não há avaliações
- 5e Lesson Plan Science Landslides FinalDocumento5 páginas5e Lesson Plan Science Landslides Finalapi-353125335Ainda não há avaliações
- Brittania Crash Winkton 1958Documento4 páginasBrittania Crash Winkton 1958droshkyAinda não há avaliações
- Safer CitiesDocumento8 páginasSafer CitiesChinmai HemaniAinda não há avaliações
- Tugas Bahasa InggrisDocumento2 páginasTugas Bahasa InggrisGanryuAinda não há avaliações
- Friends of The Boundary Waters 2014 Annual ReportDocumento8 páginasFriends of The Boundary Waters 2014 Annual ReportFriends of the Boundary Waters WildernessAinda não há avaliações
- Disaster Risk Reduction and EducationDocumento3 páginasDisaster Risk Reduction and EducationZin Maung TunAinda não há avaliações
- Lao PDR School Construction GuidelinesDocumento100 páginasLao PDR School Construction Guidelinesبشير حيدرAinda não há avaliações
- Journal Pre-Proof: Sustainable Cities and SocietyDocumento44 páginasJournal Pre-Proof: Sustainable Cities and SocietyhenryAinda não há avaliações
- Columbia Water and FEMA Come To Fundamental Agreement On Scope of Canal WorkDocumento1 páginaColumbia Water and FEMA Come To Fundamental Agreement On Scope of Canal WorkWIS Digital News StaffAinda não há avaliações
- Republic of Turkey Gaziantep University Graduate School of Natural & Applied SciencesDocumento104 páginasRepublic of Turkey Gaziantep University Graduate School of Natural & Applied SciencesCanerAinda não há avaliações
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineAinda não há avaliações
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsNo EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsNota: 4.5 de 5 estrelas4.5/5 (6)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicAinda não há avaliações
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisNo EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (9)
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthNo EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthNota: 4 de 5 estrelas4/5 (7)
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNo EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthAinda não há avaliações
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedAinda não há avaliações
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryNo EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryNota: 4 de 5 estrelas4/5 (6)
- Sickening: How Big Pharma Broke American Health Care and How We Can Repair ItNo EverandSickening: How Big Pharma Broke American Health Care and How We Can Repair ItNota: 4 de 5 estrelas4/5 (9)
- The Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeNo EverandThe Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeNota: 3.5 de 5 estrelas3.5/5 (7)
- The Inescapable Immune Escape PandemicNo EverandThe Inescapable Immune Escape PandemicNota: 5 de 5 estrelas5/5 (1)
- War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicNo EverandWar on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicNota: 4 de 5 estrelas4/5 (7)
- Microbiological Quality of FoodsNo EverandMicrobiological Quality of FoodsL SlanetzAinda não há avaliações
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"No EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Nota: 3.5 de 5 estrelas3.5/5 (3)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceNo EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceNota: 4.5 de 5 estrelas4.5/5 (15)
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadNo EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadNota: 4.5 de 5 estrelas4.5/5 (3)
- Epidemics and Society: From the Black Death to the PresentNo EverandEpidemics and Society: From the Black Death to the PresentNota: 4.5 de 5 estrelas4.5/5 (9)
- Arthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefNo EverandArthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefAinda não há avaliações
- Make America Healthy Again: How Bad Behavior and Big Government Caused a Trillion-Dollar CrisisNo EverandMake America Healthy Again: How Bad Behavior and Big Government Caused a Trillion-Dollar CrisisAinda não há avaliações
- The Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusNo EverandThe Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusNota: 4.5 de 5 estrelas4.5/5 (10)
- The Gut-loving Cookbook: Over 65 deliciously simple, gut-friendly recipes from The Gut StuffNo EverandThe Gut-loving Cookbook: Over 65 deliciously simple, gut-friendly recipes from The Gut StuffAinda não há avaliações
- Panic Attack: Playing Politics with Science in the Fight Against COVID-19No EverandPanic Attack: Playing Politics with Science in the Fight Against COVID-19Nota: 4.5 de 5 estrelas4.5/5 (10)