Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Fisiologia de KatzDocumento663 páginasFisiologia de KatzOscar Gascon100% (1)
- Exp 1 - Basic Fluid PropertiesDocumento12 páginasExp 1 - Basic Fluid PropertiesJulia FlorencioAinda não há avaliações
- Cerebral Palsy Revalida FormatDocumento10 páginasCerebral Palsy Revalida FormatChelsea CalanoAinda não há avaliações
- Buteyko Breathing Guide PDFDocumento1 páginaButeyko Breathing Guide PDFFreddy Rafael Rosales HernandezAinda não há avaliações
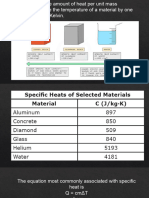
- WK 7 Specific HeatDocumento5 páginasWK 7 Specific HeatJulia FlorencioAinda não há avaliações
- Group 4 RA 9184 Articles 16-20 (TECHNOPRENEURSHIP 101 - BSCE 4-YA-1)Documento26 páginasGroup 4 RA 9184 Articles 16-20 (TECHNOPRENEURSHIP 101 - BSCE 4-YA-1)Julia FlorencioAinda não há avaliações
- Composition and Structure of The AtmosphereDocumento47 páginasComposition and Structure of The AtmosphereJulia FlorencioAinda não há avaliações
- Chemistry of Water 1Documento32 páginasChemistry of Water 1Julia FlorencioAinda não há avaliações
- WK13 - Chemistry of Atmosphere - D03Documento44 páginasWK13 - Chemistry of Atmosphere - D03Julia FlorencioAinda não há avaliações
- Program of The Civil Engineering Licensure Examination To Be Given in The Cities of Manila, Baguio, Cagayan de Oro, Cebu, IloiDocumento4 páginasProgram of The Civil Engineering Licensure Examination To Be Given in The Cities of Manila, Baguio, Cagayan de Oro, Cebu, IloiJulia FlorencioAinda não há avaliações
- Specimen Date of Casting Date of Testing Flexural Strength, Mpa 1St 2Nd 3Rd Sample NoDocumento6 páginasSpecimen Date of Casting Date of Testing Flexural Strength, Mpa 1St 2Nd 3Rd Sample NoJulia FlorencioAinda não há avaliações
- Weekly Site Inspection Report: Poi/ MTF Poi/ MTFDocumento5 páginasWeekly Site Inspection Report: Poi/ MTF Poi/ MTFJulia FlorencioAinda não há avaliações
- SNSTP Module 4 Practice #1: Iii. Planning and ApplicationDocumento3 páginasSNSTP Module 4 Practice #1: Iii. Planning and ApplicationJulia FlorencioAinda não há avaliações
- Item No. Materials UOM QTY RemarksDocumento4 páginasItem No. Materials UOM QTY RemarksJulia FlorencioAinda não há avaliações
- First Aid:: Head and Spine InjuryDocumento14 páginasFirst Aid:: Head and Spine InjuryJulia FlorencioAinda não há avaliações
- Cost Estimate For ManuscriptDocumento8 páginasCost Estimate For ManuscriptJulia FlorencioAinda não há avaliações
- P1 - Florencio, JuliaDocumento2 páginasP1 - Florencio, JuliaJulia FlorencioAinda não há avaliações
- 1 PDFDocumento1 página1 PDFJulia FlorencioAinda não há avaliações
- FSTLDSL Steel Design - Drafting: National University - ManilaDocumento5 páginasFSTLDSL Steel Design - Drafting: National University - ManilaJulia FlorencioAinda não há avaliações
- CONSTY Case StudyDocumento4 páginasCONSTY Case StudyJulia FlorencioAinda não há avaliações
- Kislev G LatestDocumento1 páginaKislev G LatestJulia FlorencioAinda não há avaliações
- Unit 3 Lateral Earth Pressure1Documento19 páginasUnit 3 Lateral Earth Pressure1Julia FlorencioAinda não há avaliações
- Cmat AssignmentDocumento7 páginasCmat AssignmentJulia FlorencioAinda não há avaliações
- Table of ContentDocumento1 páginaTable of ContentJulia FlorencioAinda não há avaliações
- NBCP Chapter 1-4Documento10 páginasNBCP Chapter 1-4Julia Florencio100% (1)
- Basic Health ServicesDocumento2 páginasBasic Health ServicesSam Raven AndresAinda não há avaliações
- Vitamin K Administration in The Newborn GuidelineDocumento10 páginasVitamin K Administration in The Newborn GuidelineAna Sarah KurniaAinda não há avaliações
- Lecture - 1 Introduction To PharmacologyDocumento62 páginasLecture - 1 Introduction To PharmacologyAshique FarhadAinda não há avaliações
- Photodynamic TherapyDocumento5 páginasPhotodynamic TherapyPranav UpadhyayaAinda não há avaliações
- NCP TractionDocumento9 páginasNCP TractionAnneSitjar100% (1)
- EMG Assisted Migraine TherapyDocumento6 páginasEMG Assisted Migraine TherapyTaufeeq Malik100% (1)
- Mechanics of Circular Breathing in Wind MusiciansDocumento8 páginasMechanics of Circular Breathing in Wind MusiciansjwmmdAinda não há avaliações
- CHECKLIST Trach Care and Suctioning.Documento6 páginasCHECKLIST Trach Care and Suctioning.Mickey MoraAinda não há avaliações
- HCVDocumento33 páginasHCVsherif555Ainda não há avaliações
- Compassion Fatigue: Caring For The CaregiverDocumento24 páginasCompassion Fatigue: Caring For The CaregiverSLCNtc75% (4)
- Functional Results of Cataract Surgery in The Treatment of Phacomorphic GlaucomaDocumento5 páginasFunctional Results of Cataract Surgery in The Treatment of Phacomorphic Glaucomachindy sulistyAinda não há avaliações
- Folder - OasisDocumento2 páginasFolder - Oasisbiomedical_com_brAinda não há avaliações
- Ranitidine 50mg - 2ml Solution For Injection and Infusion - (EMC) Print FriendlyDocumento6 páginasRanitidine 50mg - 2ml Solution For Injection and Infusion - (EMC) Print FriendlyDewi Wara ShintaAinda não há avaliações
- QC Delta PV PPT Student 09Documento8 páginasQC Delta PV PPT Student 09Susianna RismandaAinda não há avaliações
- 940837-000001 LMA-Protector Factsheet 1604Documento2 páginas940837-000001 LMA-Protector Factsheet 1604nanang criztaAinda não há avaliações
- Arterial Blood Gas UpdatedDocumento30 páginasArterial Blood Gas UpdatedMoustafa IbrahimAinda não há avaliações
- Inverted Nipples PDFDocumento2 páginasInverted Nipples PDFfifahcantikAinda não há avaliações
- AU-poster - Contact Investigation - Indonesia - 4.1Documento1 páginaAU-poster - Contact Investigation - Indonesia - 4.1Eva Tirtabayu HasriAinda não há avaliações
- Cardiac Tamponade 2Documento23 páginasCardiac Tamponade 2Jethro Floyd QuintoAinda não há avaliações
- What Did Freud Get RightDocumento3 páginasWhat Did Freud Get RightGustavo AvendañoAinda não há avaliações
- Surgical Site Infection: Dr. Maryam. Surgical Unit 3Documento22 páginasSurgical Site Infection: Dr. Maryam. Surgical Unit 3med stuAinda não há avaliações
- Post Gastrectomy SyndromeDocumento34 páginasPost Gastrectomy SyndromeWasim R. IssaAinda não há avaliações
- Procedure Checklist With Rating Form Donning and Removing Sterile GlovesDocumento4 páginasProcedure Checklist With Rating Form Donning and Removing Sterile GlovesRachel VillanuevaAinda não há avaliações
- Introduction To AnaesthesiaDocumento24 páginasIntroduction To AnaesthesiaDeobrat DwivediAinda não há avaliações
- Chronic Venous Insufficiency: A Frequently Underdiagnosed and Undertreated PathologyDocumento3 páginasChronic Venous Insufficiency: A Frequently Underdiagnosed and Undertreated PathologyWidyaSaraswatiAinda não há avaliações
- Antibiotic Classification & Mechanism - Basic Science - OrthobulletsDocumento7 páginasAntibiotic Classification & Mechanism - Basic Science - OrthobulletsYuttapol PimpisonAinda não há avaliações
- Session #2 SAS - Funda (Lec)Documento8 páginasSession #2 SAS - Funda (Lec)Mary Maxiluch TabudlongAinda não há avaliações