Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- CSS All Notes GKDocumento179 páginasCSS All Notes GKharris ghauriAinda não há avaliações
- QuestionsDocumento3 páginasQuestionsshone123Ainda não há avaliações
- Dengue Hemorrhagic Fever e A Systemic Literature Review of Current Perspectives On Pathogenesis, Prevention and ControlDocumento16 páginasDengue Hemorrhagic Fever e A Systemic Literature Review of Current Perspectives On Pathogenesis, Prevention and ControlAinun Jariah MuliadiAinda não há avaliações
- Endometriosis NEJM 2020 PDFDocumento13 páginasEndometriosis NEJM 2020 PDFluis medinaAinda não há avaliações
- Drug Resistance in Bacteria Fungi Malaria PDFDocumento629 páginasDrug Resistance in Bacteria Fungi Malaria PDFShridhar Chame100% (1)
- Syllabus PDFDocumento253 páginasSyllabus PDFVivek KumarAinda não há avaliações
- ArginineDocumento26 páginasArginineאנריקה שטרמר דיאטן קליניAinda não há avaliações
- Blood Type Review WorksheetDocumento2 páginasBlood Type Review WorksheetSofa100% (2)
- PsiconeuroinmunologíaDocumento10 páginasPsiconeuroinmunologíaLuis Alfredo Rosales GuerreroAinda não há avaliações
- Wa0004.Documento20 páginasWa0004.Mayra AlejandraAinda não há avaliações
- Imun ResponseDocumento9 páginasImun ResponsePena NofaAinda não há avaliações
- Innate ImmunityDocumento16 páginasInnate ImmunityikhaAinda não há avaliações
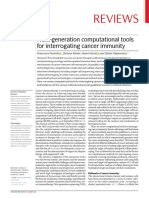
- Reviews: Next-Generation Computational Tools For Interrogating Cancer ImmunityDocumento23 páginasReviews: Next-Generation Computational Tools For Interrogating Cancer ImmunityThị Sô PhiaAinda não há avaliações
- Histology and Cell Biology An Introduction To Pathology 5Th Edition Abraham L Kierszenbaum Full ChapterDocumento67 páginasHistology and Cell Biology An Introduction To Pathology 5Th Edition Abraham L Kierszenbaum Full Chapterdennis.roberson462100% (17)
- MicrobiologyDocumento108 páginasMicrobiologyHampson Malekano100% (1)
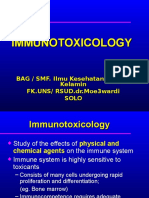
- Immunotoxicology 2007dll-2Documento80 páginasImmunotoxicology 2007dll-2Puyi PuyenkAinda não há avaliações
- Transverse Myelitis and Vaccines - A Multi-AnalysisDocumento8 páginasTransverse Myelitis and Vaccines - A Multi-AnalysisKaloy KamaoAinda não há avaliações
- Non Hodgkin Lymphoma Complete PDFDocumento104 páginasNon Hodgkin Lymphoma Complete PDFelika dwiAinda não há avaliações
- Why Women May Be Better Equipped To Fight COVIDDocumento46 páginasWhy Women May Be Better Equipped To Fight COVIDjudith retanaAinda não há avaliações
- CHAPTERS 2-4 CROSSWORD #1 SolvedDocumento4 páginasCHAPTERS 2-4 CROSSWORD #1 SolvedYu LucyAinda não há avaliações
- Human CD ChartDocumento1 páginaHuman CD ChartcoffeeaddictedAinda não há avaliações
- 2018-Pratiwi-J App Pharm SciDocumento7 páginas2018-Pratiwi-J App Pharm ScirizalAinda não há avaliações
- Complement SystemDocumento4 páginasComplement SystemFait HeeAinda não há avaliações
- DRUG STUDY (Head Injury)Documento3 páginasDRUG STUDY (Head Injury)Paula Suplico NiangarAinda não há avaliações
- Inflammation, Infection, and Microbiome in Cancers Evidence, Mechanisms, and Implications by Jun SunDocumento513 páginasInflammation, Infection, and Microbiome in Cancers Evidence, Mechanisms, and Implications by Jun SunSaiyan DianAinda não há avaliações
- Infectious Diseases: Dr. Wael H. Mansy, MD Edited by Willy ChouDocumento32 páginasInfectious Diseases: Dr. Wael H. Mansy, MD Edited by Willy Chouwildan mullerAinda não há avaliações
- Molusco ContagiosoDocumento12 páginasMolusco ContagiosoEduardo Medeiros Tabosa PinheiroAinda não há avaliações
- 10 3389@fimmu 2020 01100 PDFDocumento22 páginas10 3389@fimmu 2020 01100 PDFvalinaAinda não há avaliações
- Sofia Mubarika 180522Documento42 páginasSofia Mubarika 180522Nanik AndianiAinda não há avaliações
- AIS2 DR Daniel Nuzum Hormoneclass Detox ProtocolDocumento24 páginasAIS2 DR Daniel Nuzum Hormoneclass Detox ProtocolPanther Prime50% (2)