International Journal of Advanced Engineering Research and Science (IJAERS) [Vol-6, Issue-10, Oct- 2019]
https://dx.doi.org/10.22161/ijaers.610.23 ISSN: 2349-6495(P) | 2456-1908(O)
Cardiac physiology for biomedical engineering
Gabriela Meira de Moura Rodrigues1, Guilherme Tarcísio Leal2, Sandro
Augusto Pavlik Haddad3
1Department of electronic systems engineering and automation, University of Brasília, Brazil
Email: gabymeira@hotmail.com
2Department of biomedical engineering and automation, University of Brasília, Brazil
Email: guilhermetarcisio@iftm.edu.br
3Department of electronic systems engineering and automation, University of Brasília, Brazil
Email: sandrohaddad@gmail.com
Abstract— The multidisciplinary team provides research optimization and complementarity of ideas. Engineers
working in biomedical engineering can make your work routine easier by sharing them with healthcare
professionals who can help you understand physiology. The main objective is to address key points in cardiac
physiology and arrhythmia pathophysiology in order to lessen the efforts of biomedical engineering
professionals implementing implantable heart rate sensitive devices. It is a descriptive and critical theoretical
analysis, which selected the main and current bibliographical references, directed to the fulfillment of the main
objective. As a result, we obtained that the most important points are about the electrocardiogram graph and its
association with cardiac bioimpedance as a good physiological parameter, also about the respiratory system
that can influence cardiac health and the pathophysiology of arrhythmias that help to understand the need. to
deploy. Pacemakers. We can conclude that early identification of the gradual ST segment distance may prevent
future cardiac arrest and, in frequency-sensitive pacemakers, it is possible to identify from bioimpedance. There
is a challenge in implantable devices in differentiating between normal cardiac changes and arrhythmias, and
with the ability of biomedical engineering, the possibility of improving the performance of these devices is
always real.
Keywords— Action potential, bioimpedance, cardiovascular diseases, electrocardiogram, implantable devices.
I. INTRODUCTION produced, where analyzes and synthesis of the available
When proposing biomedical devices that influence the content in the main scientific publications on the studied
functioning of any organ, it is necessary to have a subject were performed.
minimum knowledge about its structure and behavior, so It was used as inclusion criterion of publications,
that it is possible to identify and differentiate normal current scientific texts (2015 to 2019) that contain
physiological changes from pathological changes. information that help in solving the research problem,
Working in the field of biomedical engineering, there is being excluded texts without scientific character, from
a need for both physiological and technological years before 2015 and without relevance to the theme.
knowledge, and therefore the multidisciplinary of the team
is justified. III. RESULTS AND DISCUSSION
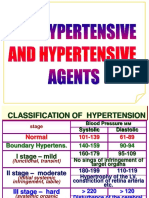
This study addresses the key points selected by a The heart is the main organ of the circulatory system
healthcare professional about heart anatomy, physiology, and has a responsibility to provide nutrients and oxygen to
biophysics, and pathophysiology in a simplified manner to each tissue through the blood. It is divided into four
facilitate understanding and work of engineering cardiac chambers, where the upper part is composed of
professionals implementing implantable heart devices, right and left atria and the lower part, right and left
particularly those that are frequency sensitive pacemakers. ventricles (Fig. 1) [1].
Typically, the implantable device electrodes are placed
II. METHODS in the right-side chambers. These chambers are separated
To answer the proposed research problem: What does a by fibrous tissue, considered a bad current conductor,
biomedical engineer need to know about heart functioning forming walls around the atrioventricular (AV) valve
in order to implement a system that helps with frequency- openings and preventing the electrical current generated by
sensitive pacemaker? A critical review of the literature was
www.ijaers.com Page | 150
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol-6, Issue-10, Oct- 2019]
https://dx.doi.org/10.22161/ijaers.610.23 ISSN: 2349-6495(P) | 2456-1908(O)
the organ itself from passing rapidly and disorderly this is one of the factors that leads to the arrhythmia
through the cardiac tissue [2]. process. In addition, there is a possibility of failure in the
production of electrical current by the SA node, triggering
the lack of chronotropism (stable heart rate).
If it occurs again, one of the predisposes is the need
for artificial pacemaker implantation. However, there are
other possibilities, one being partial or total AV node
block, His bundles or Purkinje fibers.
The action potential (AP) recorded in the ventricle is
about 105 millivolts (mV). Thus, the intracellular potential
is approximately -85mV at rest and reaches about + 20mV
during each beat. After BP onset, a membrane remains in
depolarization (with electropositive intracellular medium)
for 0.2 s, which is recorded as a plateau after
repolarization, which is the moment of return of the
intracellular medium to the negative pole [6].
Fig. 1: Anatomy of heart [3]
Action potential in the atriums is -55 to -60 mV, while
in the ventricles -85 to -90 mV. This is because sinoatrial
The left ventricular wall is thicker because it has the
fibers have a better permeability to sodium (Na +) and
function of ejecting the blood for a large circulation and,
calcium (Ca2+) ions and their positive charges counteract
therefore, the related electrocardiogram (ECG) signal may
some intracellular negativity. As this node is located in the
have a larger wavelength than the right.
atrium, electronegativity is lower in this region [7].
Cardiac behavior from the beginning of one heartbeat
Potassium ions (K+) exert a strong influence on
to the beginning of the next is called the heart cycle [4],
membrane potentials and Ca2+ act on activation of the
and from it, it is possible to obtain several parameters that,
muscle contraction mechanism. Combining both
if interpreted correctly, reveal the possible failures in your
information, it can be said that the concentration of each in
homeostasis.
the extracellular medium is essential for the cardiac
The generation of this beat occurs from the electrical
pumping process [8].
current released by the sinoatrial node or sinus node (SA),
In excess, K+ may cause myocardial dilation with
located above the right atrium, at the entrance of the
consequent sagging, reducing the frequency of beats. It can
superior vena cava (Fig. 1). The atrioventricular (AV)
also block the conduction of the atrial current towards the
node slows the pulse from the upper to the front of the
ventricles, and if this increase is two to three times beyond
ventricles and the AV beam conducts the current to the
normal concentration, it is possible that beat weakness is
lower syncytium, while Purkinje fibers distribute energy
fatal [9].
equally throughout the heart muscle tissue [5].
Excess Ca2+ has the opposite action because it induces
Some cardiac fibers are capable of self-excitation,
the myocardium to produce contraction in the form of
which facilitates the generation of rhythmic automatic
spasms. Speaking of disability, it precedes a fall similar to
discharge with consequent contractions at the same rate.
lack of K+, however, the body can maintain its levels more
Hence the ease of a single point of current generation (SA
easily without major clinical concerns [8].
node) dictating the rhythm of the entire organ [6].
Figure 2 shows the cardiac cycle events that were
If there is AV block, for example, the pulse does not
extracted based on the left side of the heart. The curve "a"
pass from the atrial syncytium to the ventricular. The atria
represents the pressure in the aorta. It can be noted that the
remain contracting with normal frequency and the ectopic
aortic valve opens at the time of systole and with its
pacemaker usually developed in the Purkinje fibers leads
pressure is increased and soon after its closure, the diastole
to ventricular muscle frequencies between 15 and 40 beats
is started and the pressure decreases.
per minute (bpm). With this sudden blockage, the Purkinje
This parameter is not directly perceived by
system takes about 5 to 20 s to react. During this time, the
implantable devices, but knowing that this opening
ventricles become bloodless and after 4-5 s due to lack of
depends on the ventricular force, if pacing is not sufficient
blood flow to the brain region, fainting and, in more severe
for the heart's blood ejection process, the ideal pressure
cases, death may occur [1].
will not be reached and the ideal blood volume will not
This property, when decompensated, can generate
come out of the ventricle.
ectopic excitation points in various parts of the tissue and
www.ijaers.com Page | 151
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol-6, Issue-10, Oct- 2019]
https://dx.doi.org/10.22161/ijaers.610.23 ISSN: 2349-6495(P) | 2456-1908(O)
Curve "b" represents atrial pressure. It is noted that the type of device as an ideal or pathological indicator of
amplitude is much smaller than that of the ventricle, functioning, mainly because it behaves synchronously with
because its structure is smaller and its wall less thick [5]. the ST segment.
Curve “c” represents ventricular pressure, approaching 120 ST segment provides information on the delay time
mmHg for aortic valve opening and blood ejection for between systole and ventricular diastole and the
large circulation [10]. If current flow to the ventricle is progressive distance between it is indicative of future
impaired, it will lose its ability to contract, which causes cardiac arrest [12]. Implantable devices do not read the
the chamber to empty. In the figure 2, ventricular volume ECG directly; However, by perceiving the cardiac
is represented on curve "d". bioimpedance signal, this parameter can be extracted and
The electrocardiogram (curve e) is composed of P used as a pathological alert.
wave, QRS complex, T wave and eventually U; which are In addition, there are other associated physiological
electrical voltages generated in the heart and recorded by conditions, such as heart rate (HR), number of beats in one
the equipment on the body surface. The P wave represents minute, and cardiac output (CO), which correspond to the
the spread of atrial depolarization. After approximately volume of blood that passes through the heart in one
0.15s, there is the QRS complex, representing ventricular minute [2].
depolarization, and then the T wave representing At rest, a healthy individual can pump 4-6 liters of
ventricular repolarization. The U wave, when identified, blood per minute and, in intense physical activity, has the
corresponds to the repolarization of the papillary muscles ability to increase this value up to seven times. This
[11]. volume control is based on the intrinsic cardiac regulation
of the variation in the amount of fluid reaching the heart
and the control of the heart rate, as well as its pumping
force, which are the responsibility of the Autonomic
Nervous System (ANS) [1].
The sympathetic and parasympathetic (or vagus)
nerves innervate myocardial tissue and are part of the
pumping effectiveness. Sympathetic stimulation can
increase cardiac output by 100%, beats usually 70 per
minute can reach 250 and increase systolic strength by up
to two times in cases of physical activity or stressful
situations such as fear.
The parasympathetic can slow down and even stop
beating for a few seconds, and then tap again 20 to 40
times per minute while vagal stimulation is stimulated, for
example, by meditation. It is important to report that, as
Fig. 2: In a) Graph of aortic pressure during the left parasympathetic fibers are more concentrated in the atria,
cardiac cycle, b) Left atrial pressure in systole and their stimulation is able to reduce HR, but not considerably
diastole, c) Left ventricular pressure in systole and the contraction force [11], considering that variations in
diastole, d) Ventricular volume in the period of relaxation cardiac output (CO) resulting from nerve stimulation
and contraction, in e) Signal electrocardiogram with the imply changes in HR and contraction force [2].
waves P, QRS and T, and in f) the left cycle When a frequency-sensitive pacemaker has the ability
phonocardiogram [1] to extract ST segment information associated with CO and
HR, it increases its reliability of accuracy when acting,
There is a delay of 0.1 s in the passage of this impulse considering the property of interpreting physiological
from the atriums to the ventricles, allowing atrial systole, changes by disease process or physical activity, as an
which brings blood to the ventricles and then ventricular example.
systole, to take blood to the organs. This delay is essential Intense physical stress requires more circulatory
so that systole does not occur at the same time in all system activity due to the need to increase blood flow to
chambers [2]. the muscles currently being exercised. Non-athletes may
Electrocardiogram graph is indispensable when it have an increase in cardiac output up to five times above
comes to heart health research and, in frequency-sensitive normal, whereas in a top athlete it reaches up to seven
pacemakers, its parameters can be used. The bioimpedance times [2].
signal, for example, is a condition that can be read by this
www.ijaers.com Page | 152
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol-6, Issue-10, Oct- 2019]
https://dx.doi.org/10.22161/ijaers.610.23 ISSN: 2349-6495(P) | 2456-1908(O)
In order to perform this special nourishment of the injury, alternative bundle branch block and other related
active tissues, the heart is stimulated by the sympathetic consequences [3].
nervous system to considerably increase its frequency and The general pathophysiology of arrhythmias is
pumping force, and in turn inhibits the parasympathetic divided into three, namely: hyperautomaticity; triggered
nervous system [3]. activity; and reentry process.
In addition, most peripheral circulation arterioles are Hyperperaeromaticity is a process represented by the
very contracted except active muscle arterioles, as they are activation and acceleration of cardiac cells that results in
very vasodilated. This is exactly why the heart needs to spontaneous depolarizations. This hyperactivity can be
respond by sending more of its supply through pumping derived from nervous system dysfunction or even fever,
blood, and the body can still redirect fluid from where it is shock, acidosis and endocrinopathies [3]. In the triggered
most needed at the moment. Interestingly enough, too, is activity, the changes are generated from the variation of
the considerable increase in systemic filling pressure that the membrane potential, which generates new action
occurs because the vein walls contract with a very potentials and, consequently, arrhythmias. This may be
powerful force [2]. due to decreased ion efflux in the cell or even increased
Sympathetic stimulation is important for the positive ion influx. The reentry process is the main reason
consequent increase in blood pressure, resulting in for ventricular and supraventricular arrhythmias. Occurs
vasoconstriction of arterioles in the body. For active by the presence of an obstacle in the anatomical structures
muscles, there is increased frequency of beats and through which the electric current is conducted [2].
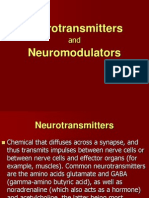
increased blood ejection pressure in the body [12]. It is possible, by observing the action potential
When an individual comes out of rest, the oxygen-rich wavelength (Fig. 3), to identify if there are pathological
blood supply must be increased to nourish the muscles changes in the current conduction. The formula consists
used. The more circulation needed, the greater the cardiac of: Wavelength = Conduction Speed x Refractory Period.
output (how much blood circulates in the heart per minute) Thus, when the wavelength exceeds the anatomical size of
and pulmonary ventilation [1]. Heart rate changes isolated the circuit, the arrhythmia is extinguished. And if the
from ventilatory behavior indicate pathological process wavelength is shorter than the arrhythmic circuit, the
that should be researched. arrhythmia will be maintained [6].
Cardiac contraction force can be increased by
elevating the temperature by physical activity. However, in
states where the condition continues, such as fever, HR
can bend and deplete metabolic systems, causing
weakness. If hypothermia occurs, consequently there is a
reduction in this frequency, which can lead to death [12].
Outside of physical activity, there is still the
possibility of the heart manifesting inappropriate behavior.
When such events occur frequently and are correctly
diagnosed, the cardiologist may consider it necessary to
implant an artificial pacemaker to assist in the process of
induced activity regularization and, consequently, to
increase life expectancy.
Cardiovascular disease is the leading cause of death
from disease worldwide, with an estimated 17.7 million Fig. 3: Heart action potential
deaths in 2015 (31% worldwide) and 17.9 million in 2016 With this graph it is possible to visualize the moments
(44% worldwide). In addition, more than 75% of these of depolarization (0), rapid and incomplete repolarization
occurred in low-income and middle-income countries [13]. (1), plateau moment (2), depolarization (3) and electrical
The main clinical features of arrhythmias required for diastole (4), thus completing a cardiac cycle.
pacemaker implantation are: hypersensitive carotid
syndrome, neurocardiogenic syncope, SA node disease, IV. CONCLUSION
non-drug-responsive bradycardic syndrome, ventricular It is a fact that there is much more complex
control atrial fibrillation, AV-grade AV block, and second- information, from the anatomy to the pathophysiology of
degree type. II AV, advanced AV block, fiber bundle arrhythmias, however, with the information present in this
text, after a practical observation of the difficulties
www.ijaers.com Page | 153
International Journal of Advanced Engineering Research and Science (IJAERS) [Vol-6, Issue-10, Oct- 2019]
https://dx.doi.org/10.22161/ijaers.610.23 ISSN: 2349-6495(P) | 2456-1908(O)
encountered by biomedical engineers in the development [13] OPAS. Doenças cardiovasculares. 2017. Disponível em:
of this type of project, it is believed to be sufficient to https://www.paho.org/bra/index.php?option=com_content&
facilitate understanding of heart function and propose view=article&id=5253:doencas-
cardiovasculares&Itemid=1096. Accessed in October 11,
technologies that can solve pathological problems.
2019.
One of the main points that deserves due attention is
[14] Ikonnikov, G., Yelle, D. (2013). Physiology of cardiac
the early identification of ST segment detachment on the contraction and contractility. Available at: http://
electrocardiogram, as it may prevent future cardiac arrest. www.pathophys.org/physiology-of-cardiac-conduction-and-
When it comes to frequency-sensitive pacemakers, this contractility/#Electrophysiology. Accessed in October 11,
behavior can be identified by reading the bioimpedance. 2019.
Getting the implantable device to identify when cardiac
change occurs due to normal day conditions or
pathological disorders is always a challenge. However,
with the ability of biomedical engineering, the possibility
of improving the performance of these devices is always
real.
REFERENCES
[1] Guyton, A.C. e Hall, J.E. (2017). Tratado de fisiologia
médica, 13rd ed. Rio de Janeiro: Elsevier, 1168p.
[2] Berne, R.M e Levy, M.N. (2018). FIsiologia. 7th ed, vol. 7.
Rio de Janeiro: Elsevier, 880p.
[3] Mc Graw-Hill. Available in: https://br.pinterest.com/.
Accessed in October 11, 2019.
[4] Vanputte, C.L., Regan, J.L. e Russo, A.F. (2016). Anatomia
e fisiologia de seeley.10th ed. Porto Alegre: Artmed, 1264p.
[5] Boron, W.F. e Boulpaep, E.L. (2017). Medical physiology.
3st ed. Philadelphia: Elsevier, 1312p.
[6] Duran, J.E.R. (2015). Biofísica conceitos e aplicações.2nd
ed. Pearson, 320p.
[7] Gandon-Renard, M., Bedioune, I., Karam, S., Varin, A.,
Lechène, P., Bichali, S., Leroy, J., Algalarrondo, V.,
Stratakis, C., Mercadier, J.J., Benitah, J.P., Gomez, A.M.,
Fischmeinster, R. e Vandecasteele, G. (2019). The cAMP-
dependent protein kinase type, I regulates cardiac excitation-
contration coupling. Archives of Cardiovascular Diseases
Supplements (ISSN 1878-6480), 11(2), 261-266.
https://www.sciencedirect.com/journal/archives-of-
cardiovascular-diseases-supplements
[8] Catterall, W, Lenaeus, J, El-Din, T.M. (2019). Structure and
pharmacology of voltage-gated sodium and calcium
channels. Annual Review of Pharmacology and Toxicology
(ISSN 1545-4304). https://doi.org/10.1146/annuarey-
pharmtox-010818-021757.
[9] Guerri, G., Krasi, G., Precone, V., Paolacci, S., Chiurazzi,
P., Arrigoni, L., Cortese, B., Dautaj, A., Bertelli, M. (2019).
Cardiac conduction defects. Acta Biomed (30(10), 20-29).
DOI: 10.23750/abm.v90i10-S.8751
[10] Silverthorn, D.U. (2017). Fisiologia humana: uma
abordagem integrada. 7th ed. Porto Alegre: Artmed, 960p.
[11] Santos, J.L.F. (2016). Eletrocardiograma ao alcance de
todos. 3rd ed. São Paulo: Phorte, 176p.
[12] Timperley, J., Leeson, P., Mirchell, A. R. J., Betts, T.
(2019). Cardiology pacemakers and ICDs. 2nd ed. Oxford
Medical Publications, 7109p.
www.ijaers.com Page | 154
Você também pode gostar
- 247 FullDocumento6 páginas247 FullBryan FarrelAinda não há avaliações
- 38.17 Cardiac Pacing: Basic Concepts: Renato Pietro RicciDocumento16 páginas38.17 Cardiac Pacing: Basic Concepts: Renato Pietro RicciurtikikeAinda não há avaliações
- Fundamentals of ECG InterpretationDocumento12 páginasFundamentals of ECG InterpretationPankaj Patil100% (1)
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXNo EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXNota: 5 de 5 estrelas5/5 (2)
- Restoring Heart Function and Electrical IntegrityDocumento13 páginasRestoring Heart Function and Electrical IntegrityRaul OrtegaAinda não há avaliações
- Myatricle 3Documento9 páginasMyatricle 3HIROMY EMMY HERRERA MENDOZAAinda não há avaliações
- Cardiac PacemakersDocumento206 páginasCardiac PacemakersMiguel PenarandaAinda não há avaliações
- 1 s2.0 S0169260714001485 MainDocumento10 páginas1 s2.0 S0169260714001485 MainJhon Bairon Velásquez MiraAinda não há avaliações
- Sitabhra Sinha Et Al - Critical Role of Inhomogeneities in Pacing Termination of Cardiac ReentryDocumento10 páginasSitabhra Sinha Et Al - Critical Role of Inhomogeneities in Pacing Termination of Cardiac ReentryGretymjAinda não há avaliações
- 1 s2.0 S2405844023000944 MainDocumento25 páginas1 s2.0 S2405844023000944 MainUli Urio-LegoAinda não há avaliações
- Sinusnodedysfunction: Neeraj Sathnur,, Emanuel Ebin,, David G. BendittDocumento19 páginasSinusnodedysfunction: Neeraj Sathnur,, Emanuel Ebin,, David G. Bendittnicolas.sierra1Ainda não há avaliações
- 24junctional Ectopic TachycardiaDocumento3 páginas24junctional Ectopic TachycardiaZiedTrikiAinda não há avaliações
- Comparison of PSD of Normal and Abnormal ECGsDocumento5 páginasComparison of PSD of Normal and Abnormal ECGsEduardoHernandezAinda não há avaliações
- Basic Surface Electrocardiogram Interpretation For The PharmacistDocumento12 páginasBasic Surface Electrocardiogram Interpretation For The PharmacistFelipe SotoAinda não há avaliações
- Electrocardiogram (ECG/EKG) : Topic OutlineDocumento5 páginasElectrocardiogram (ECG/EKG) : Topic OutlineDan Dan ManaoisAinda não há avaliações
- Diagnosis and Management Sudden Cardiac Death 2005Documento7 páginasDiagnosis and Management Sudden Cardiac Death 2005aminceloAinda não há avaliações
- Interpretation of The Electrocardiogram - Part IV - The ST Segment, T and U Waves, and The QT IntervalDocumento10 páginasInterpretation of The Electrocardiogram - Part IV - The ST Segment, T and U Waves, and The QT Intervallu truongAinda não há avaliações
- ECG Monitoring in TheatreDocumento17 páginasECG Monitoring in TheatrePhani NadellaAinda não há avaliações
- 19 Vol 92 No 1Documento9 páginas19 Vol 92 No 1lahlouhAinda não há avaliações
- Pacemakers and Implantable Cardioverter DefibrillatorsDocumento10 páginasPacemakers and Implantable Cardioverter Defibrillatorsnoorhadi.n10Ainda não há avaliações
- Antiarrhythmicdrugs: Risks and BenefitsDocumento14 páginasAntiarrhythmicdrugs: Risks and Benefitsreinaldo valdes iznagaAinda não há avaliações
- Electrocardiography II StudentDocumento20 páginasElectrocardiography II StudentArmando Valdez ZamoranoAinda não há avaliações
- Ni Hms 589535Documento26 páginasNi Hms 589535Sara TeixeiraAinda não há avaliações
- Modern Concepts Concerning The Origin Physiol.00054.2012Documento19 páginasModern Concepts Concerning The Origin Physiol.00054.2012Pedro RodriguezAinda não há avaliações
- Logy Assighnment On Automaticity Rhythmicity AutorecoveredDocumento10 páginasLogy Assighnment On Automaticity Rhythmicity AutorecoveredM Asif RiazAinda não há avaliações
- Cardiac Arrhythmia Classification Using Boosted Decision TreesDocumento11 páginasCardiac Arrhythmia Classification Using Boosted Decision TreesShweta RaoAinda não há avaliações
- A Protocol For Transverse Cardiac Slicing and Optical Mapping in Murine HeartDocumento8 páginasA Protocol For Transverse Cardiac Slicing and Optical Mapping in Murine HeartMaria Perez ZabalzaAinda não há avaliações
- Article5 AabidDocumento9 páginasArticle5 AabidlahlouhAinda não há avaliações
- (Journal Q2 2023) Heart Arrhythmia Detection and Classification A Comparative StudyDocumento21 páginas(Journal Q2 2023) Heart Arrhythmia Detection and Classification A Comparative StudyVideo GratisAinda não há avaliações
- Application of Nuclear Magnetic Resonance ImagingDocumento19 páginasApplication of Nuclear Magnetic Resonance ImagingHoracio Dorantes ReyesAinda não há avaliações
- EJMSOL14Documento10 páginasEJMSOL14Sara TeixeiraAinda não há avaliações
- Mechanisms of Cardiac Arrhythmias: Larraitz Gaztan Aga, Francis E. Marchlinski, and Brian P. BetenskyDocumento12 páginasMechanisms of Cardiac Arrhythmias: Larraitz Gaztan Aga, Francis E. Marchlinski, and Brian P. BetenskyAída FernandaAinda não há avaliações
- Major Project Phase 1 Report CloudDocumento35 páginasMajor Project Phase 1 Report CloudPraj CAinda não há avaliações
- Marchant2022 CardiacPacemakerAPDocumento7 páginasMarchant2022 CardiacPacemakerAPsabrinasameja75Ainda não há avaliações
- Biomedical Signal Processing and ControlDocumento10 páginasBiomedical Signal Processing and ControlSERGIO ANDRES ROMERO TORRESAinda não há avaliações
- Medical Electronics - SKP 116 135Documento20 páginasMedical Electronics - SKP 116 135Mohammed Mian AAinda não há avaliações
- Interpreting AV (Heart) Blocks: Breaking Down The Mystery: 2 Contact HoursDocumento29 páginasInterpreting AV (Heart) Blocks: Breaking Down The Mystery: 2 Contact HoursAsri RachmawatiAinda não há avaliações
- Clinical Handbook of Cardiac ElectrophysiologyNo EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverAinda não há avaliações
- 3381-Article Text-17320-2-10-20220224Documento9 páginas3381-Article Text-17320-2-10-20220224Maja MitreskaAinda não há avaliações
- How To: A Practical Guide To Cardiac Conduction Devices On Chest RadiographDocumento7 páginasHow To: A Practical Guide To Cardiac Conduction Devices On Chest RadiographAndreea TeodorescuAinda não há avaliações
- Arritmia SVDocumento17 páginasArritmia SVCésar Lobo TarangoAinda não há avaliações
- A Brief Review History To Understand Fundamentals of ElectrocardiographyDocumento6 páginasA Brief Review History To Understand Fundamentals of ElectrocardiographyAbdullah AbdurrehmanAinda não há avaliações
- IEEEDocumento5 páginasIEEESanjana GururajAinda não há avaliações
- Computer SimulationDocumento29 páginasComputer SimulationmrtiborhornyikAinda não há avaliações
- 9a61527a3a71b7c Ek PDFDocumento5 páginas9a61527a3a71b7c Ek PDFMd Abdul RahemanAinda não há avaliações
- Voltage Noise in Uences Action Potential Duration in Cardiac MyocytesDocumento22 páginasVoltage Noise in Uences Action Potential Duration in Cardiac MyocytesAndres CampoAinda não há avaliações
- The Evolution of PacemakersDocumento11 páginasThe Evolution of PacemakersAman PotdarAinda não há avaliações
- Cardiac PacingDocumento9 páginasCardiac PacingmatzoneAinda não há avaliações
- EXS 212 Lab 2: Electrocardiogram: ObjectivesDocumento5 páginasEXS 212 Lab 2: Electrocardiogram: ObjectivesAnonymous CHVzVzf3uRAinda não há avaliações
- Nihms 992969Documento26 páginasNihms 992969aliusman laseAinda não há avaliações
- 1 s2.0 S0006291X19309039 MainDocumento6 páginas1 s2.0 S0006291X19309039 MainJeniffer VillamilAinda não há avaliações
- Myarticle 2Documento6 páginasMyarticle 2mypinklagoon8411Ainda não há avaliações
- Using The 12-Lead ECG To Localize The Origin of Atrial and Ventricular Tachycardias. Part 2-Ventricular TachycardiaDocumento9 páginasUsing The 12-Lead ECG To Localize The Origin of Atrial and Ventricular Tachycardias. Part 2-Ventricular Tachycardiarentedmule00Ainda não há avaliações
- Unit 4 (7) Origin and Conduction of Cardiac ImpulsesDocumento31 páginasUnit 4 (7) Origin and Conduction of Cardiac ImpulsesDINAMANI 0inamAinda não há avaliações
- Applsci 11 06622Documento19 páginasApplsci 11 06622Maria Jose Quishpe GuachalaAinda não há avaliações
- ECG EquinoDocumento19 páginasECG EquinoAgro PetAinda não há avaliações
- Cardiac Electrophysiology Without FluoroscopyNo EverandCardiac Electrophysiology Without FluoroscopyRiccardo ProiettiAinda não há avaliações
- Tissue To Organisms/Physiology & PharmacologyDocumento6 páginasTissue To Organisms/Physiology & PharmacologyStudent LifeAinda não há avaliações
- Decoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonNo EverandDecoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonAfzal SohaibAinda não há avaliações
- Facing Dengue and Malaria As A Public Health Challenge in BrazilDocumento6 páginasFacing Dengue and Malaria As A Public Health Challenge in BrazilIJAERS JOURNALAinda não há avaliações
- Enhancing Cybersecurity: The Power of Artificial Intelligence in Threat Detection and PreventionDocumento6 páginasEnhancing Cybersecurity: The Power of Artificial Intelligence in Threat Detection and PreventionIJAERS JOURNALAinda não há avaliações
- The Economic Impact of Coronavirus Disease (COVID-19) : A Study On Tourism Indicators in The Kingdom of Saudi ArabiaDocumento4 páginasThe Economic Impact of Coronavirus Disease (COVID-19) : A Study On Tourism Indicators in The Kingdom of Saudi ArabiaIJAERS JOURNALAinda não há avaliações
- Impacts On The Mental Health of Professionals in A Prisonal System in Alagoas During The Covid-19 PandemicDocumento7 páginasImpacts On The Mental Health of Professionals in A Prisonal System in Alagoas During The Covid-19 PandemicIJAERS JOURNALAinda não há avaliações
- Business Logistics and The Relationship With Organizational SuccessDocumento4 páginasBusiness Logistics and The Relationship With Organizational SuccessIJAERS JOURNALAinda não há avaliações
- Climatic Rhythms and Prevalence of Malaria in The Municipality of Sinende in Northern BeninDocumento8 páginasClimatic Rhythms and Prevalence of Malaria in The Municipality of Sinende in Northern BeninIJAERS JOURNALAinda não há avaliações
- Beef Cattle Farmers' Economic Behavior in The Minahasa Tenggara Regency, IndonesiaDocumento7 páginasBeef Cattle Farmers' Economic Behavior in The Minahasa Tenggara Regency, IndonesiaIJAERS JOURNALAinda não há avaliações
- The Economic Impact of Coronavirus Disease (COVID-19) : A Study On Tourism Indicators in The Kingdom of Saudi ArabiaDocumento4 páginasThe Economic Impact of Coronavirus Disease (COVID-19) : A Study On Tourism Indicators in The Kingdom of Saudi ArabiaIJAERS JOURNALAinda não há avaliações
- Study of The Extraction Process of The Pleurotus Citrinopileatus Mushroom and Evaluation of The Biological Activity of The ExtractDocumento8 páginasStudy of The Extraction Process of The Pleurotus Citrinopileatus Mushroom and Evaluation of The Biological Activity of The ExtractIJAERS JOURNALAinda não há avaliações
- Associativism As Strategy of Reaching Territorial Rights, Programs, Projects and Public Policies of Rural Development: The Case of The São Francisco Do Mainã Community, Manaus, AMDocumento9 páginasAssociativism As Strategy of Reaching Territorial Rights, Programs, Projects and Public Policies of Rural Development: The Case of The São Francisco Do Mainã Community, Manaus, AMIJAERS JOURNALAinda não há avaliações
- Analysis of The Thermal Behavior of Masonry Concrete Block With Internal Natural Element CoatingDocumento11 páginasAnalysis of The Thermal Behavior of Masonry Concrete Block With Internal Natural Element CoatingIJAERS JOURNALAinda não há avaliações
- Constructed Wetlands: Technology For Removing Drug Concentration From WaterDocumento12 páginasConstructed Wetlands: Technology For Removing Drug Concentration From WaterIJAERS JOURNALAinda não há avaliações
- Breastfeeding and Factors Associated With The Prevention of Childhood Obesity: An Integrative Literature ReviewDocumento16 páginasBreastfeeding and Factors Associated With The Prevention of Childhood Obesity: An Integrative Literature ReviewIJAERS JOURNALAinda não há avaliações
- Water Quality Assessment Using GIS Based Multi-Criteria Evaluation (MCE) and Analytical Hierarchy Process (AHP) Methods in Yenagoa Bayelsa State, NigeriaDocumento11 páginasWater Quality Assessment Using GIS Based Multi-Criteria Evaluation (MCE) and Analytical Hierarchy Process (AHP) Methods in Yenagoa Bayelsa State, NigeriaIJAERS JOURNALAinda não há avaliações
- Process Sequence Optimization and Structural Analysis of Nanoscale Heterostructure Using Compound Semiconductors AlAsSb/In0.59Ga0.41As/GaAs0.53Sb0.47Documento5 páginasProcess Sequence Optimization and Structural Analysis of Nanoscale Heterostructure Using Compound Semiconductors AlAsSb/In0.59Ga0.41As/GaAs0.53Sb0.47IJAERS JOURNALAinda não há avaliações
- Childhood/ Pediatric Cancer: Nursing Care in Oncopediatrics With A Central Focus On HumanizationDocumento12 páginasChildhood/ Pediatric Cancer: Nursing Care in Oncopediatrics With A Central Focus On HumanizationIJAERS JOURNALAinda não há avaliações
- VCO Rancidity Analysis Refers To Fermentation Time That Produced by Gradual Heating MethodDocumento6 páginasVCO Rancidity Analysis Refers To Fermentation Time That Produced by Gradual Heating MethodIJAERS JOURNAL100% (1)
- Komla Uwolowudu Amegna: International Journal of Advanced Engineering Research and Science (IJAERS)Documento9 páginasKomla Uwolowudu Amegna: International Journal of Advanced Engineering Research and Science (IJAERS)IJAERS JOURNALAinda não há avaliações
- Sociodemographic and Clinical Profile of Women With Uterine Cervical Cancer Attended in An Oncological Hospital in The State of Acre, BrazilDocumento9 páginasSociodemographic and Clinical Profile of Women With Uterine Cervical Cancer Attended in An Oncological Hospital in The State of Acre, BrazilIJAERS JOURNALAinda não há avaliações
- Design and Building of Servo Motor Portable Coconut Peller MachineDocumento5 páginasDesign and Building of Servo Motor Portable Coconut Peller MachineIJAERS JOURNALAinda não há avaliações
- Morphometric Analysis of The Ekole River As A Consequence of Climate Change: A Case Study in Yenagoa, Bayelsa State, NigeriaDocumento9 páginasMorphometric Analysis of The Ekole River As A Consequence of Climate Change: A Case Study in Yenagoa, Bayelsa State, NigeriaIJAERS JOURNALAinda não há avaliações
- Multiprofessional Care For A Patient With Gestational DiabetesDocumento12 páginasMultiprofessional Care For A Patient With Gestational DiabetesIJAERS JOURNALAinda não há avaliações
- Morphometric Analysis of The Ekole River As A Consequence of Climate Change: A Case Study in Yenagoa, Bayelsa State, NigeriaDocumento9 páginasMorphometric Analysis of The Ekole River As A Consequence of Climate Change: A Case Study in Yenagoa, Bayelsa State, NigeriaIJAERS JOURNALAinda não há avaliações
- Association of Bacterial Vaginosis To Atypia in Squamous Cells of The CervixDocumento15 páginasAssociation of Bacterial Vaginosis To Atypia in Squamous Cells of The CervixIJAERS JOURNALAinda não há avaliações
- Mining and Its Impacts On Environment and Health With Special Reference To Ballari District, Karnataka, IndiaDocumento7 páginasMining and Its Impacts On Environment and Health With Special Reference To Ballari District, Karnataka, IndiaIJAERS JOURNALAinda não há avaliações
- Assessment of The Risk of Cardiovascular Diseases and Its Relationship With Heart Rate Variability in Physically Active and Sedentary IndividualsDocumento13 páginasAssessment of The Risk of Cardiovascular Diseases and Its Relationship With Heart Rate Variability in Physically Active and Sedentary IndividualsIJAERS JOURNALAinda não há avaliações
- Modeling of Geological and Geophysical Data, Onshore Field of Potiguar Basin, Northeastern BrazilDocumento5 páginasModeling of Geological and Geophysical Data, Onshore Field of Potiguar Basin, Northeastern BrazilIJAERS JOURNALAinda não há avaliações
- Humanization in Undergraduate Medical Education: The Brazilian Learner's PerspectiveDocumento12 páginasHumanization in Undergraduate Medical Education: The Brazilian Learner's PerspectiveIJAERS JOURNALAinda não há avaliações
- Does Blended Learning Approach Affect Madrasa Students English Writing Errors? A Comparative StudyDocumento12 páginasDoes Blended Learning Approach Affect Madrasa Students English Writing Errors? A Comparative StudyIJAERS JOURNALAinda não há avaliações
- The Psychologist's Role in The Process of Listening To Children Victims of Sexual Violence in Legal ProceedingsDocumento8 páginasThe Psychologist's Role in The Process of Listening To Children Victims of Sexual Violence in Legal ProceedingsIJAERS JOURNALAinda não há avaliações
- Neurogenic Shock in Critical Care NursingDocumento25 páginasNeurogenic Shock in Critical Care Nursingnaqib25100% (4)
- Ob NCP 2Documento2 páginasOb NCP 2Kimberly Mondala (SHS)Ainda não há avaliações
- Antihypertensive DrugsDocumento29 páginasAntihypertensive Drugsmailforrandomuse100% (1)
- Dissecting A Chicken Wing: Lab SafetyDocumento21 páginasDissecting A Chicken Wing: Lab SafetyWynona Louiz TangcoAinda não há avaliações
- The Respiratory Structure and Breathing Mechanism in AnimalsDocumento6 páginasThe Respiratory Structure and Breathing Mechanism in AnimalsNur Busyra100% (1)
- Respiratory Physiology & NeurobiologyDocumento5 páginasRespiratory Physiology & NeurobiologynimaaandmAinda não há avaliações
- Acute ST Elevation Myocardial Infarction - StatPearls - NCBI BookshelfDocumento9 páginasAcute ST Elevation Myocardial Infarction - StatPearls - NCBI BookshelfZ Siclayi AtlAinda não há avaliações
- St. Luke's College of Medicine - William H. Quasha Memorial: Block 1Documento9 páginasSt. Luke's College of Medicine - William H. Quasha Memorial: Block 1Mavic Villanueva100% (1)
- NeurotransmittersDocumento63 páginasNeurotransmittersNeelu Soni100% (1)
- Energy Expenditure and FatigueDocumento49 páginasEnergy Expenditure and FatigueAh Zhang100% (1)
- Tetanus PathoDocumento3 páginasTetanus PathoElisha Gine AndalesAinda não há avaliações
- AP Bio - Chapter 40 OutlineDocumento8 páginasAP Bio - Chapter 40 OutlineEllen LiAinda não há avaliações
- Ecmo TroubleshootingDocumento1 páginaEcmo TroubleshootingMitch ConnerAinda não há avaliações
- DigestionDocumento1 páginaDigestionPratham KamaniAinda não há avaliações
- Diabetes InsidipusDocumento2 páginasDiabetes InsidipusLena RoweAinda não há avaliações
- Heart: Petr Hajek, MD., PH.DDocumento29 páginasHeart: Petr Hajek, MD., PH.DTodesengelAinda não há avaliações
- Nervous System WSHDocumento2 páginasNervous System WSHArdra AnilAinda não há avaliações
- Anatomy of Root and StemDocumento48 páginasAnatomy of Root and StemLIONS GAMERSAinda não há avaliações
- Gap Co2 Cocc 2018Documento9 páginasGap Co2 Cocc 2018Cesar Rivas CamposAinda não há avaliações
- Current Concepts of Damage Control Resuscitation and Damage Control SurgeryDocumento52 páginasCurrent Concepts of Damage Control Resuscitation and Damage Control SurgerydewiswahyuAinda não há avaliações
- UWorld Step 2 CK Notes - 2015Documento4 páginasUWorld Step 2 CK Notes - 2015Ernesto Prado67% (3)
- Unit 1 Part 3 SignallingDocumento32 páginasUnit 1 Part 3 SignallingAnn NguyenAinda não há avaliações
- Jurnal InternationalDocumento9 páginasJurnal InternationalRulix SevenfoldAinda não há avaliações
- HS70A Reference Manual En-UsDocumento280 páginasHS70A Reference Manual En-UsVamsi ReddyAinda não há avaliações
- Human Organ Systems Lesson PlanDocumento4 páginasHuman Organ Systems Lesson PlanShaira LinalcosoAinda não há avaliações
- Bmi MCQ MarkedDocumento26 páginasBmi MCQ MarkedAbcdAinda não há avaliações
- Heart FailureDocumento41 páginasHeart FailureMatthew Jerome van HuizenAinda não há avaliações
- Walter Cannon, Homeostasis and The Physiological Response To StressDocumento12 páginasWalter Cannon, Homeostasis and The Physiological Response To StressMarc Imhotep Cray, M.D.Ainda não há avaliações
- Mod9Week3 - PA 3306 - Sept 5&6Documento22 páginasMod9Week3 - PA 3306 - Sept 5&6komal sheikhAinda não há avaliações
- Cardiovascular DiseasesDocumento67 páginasCardiovascular DiseasesokaciaAinda não há avaliações