Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Cytotoxicity of ( (E) - 1 - (4-Aminophenyl) - 3-Phenylprop-2-En-1-One) ) On Helacell LineDocumento6 páginasCytotoxicity of ( (E) - 1 - (4-Aminophenyl) - 3-Phenylprop-2-En-1-One) ) On Helacell LineWahyu Dwi NugrohoAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- 6.diabetes Education in ChilDocumento9 páginas6.diabetes Education in ChilWahyu Dwi NugrohoAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Phytosomes-A Brief OverviewDocumento7 páginasPhytosomes-A Brief OverviewWahyu Dwi NugrohoAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Antioxidants: Oxidative Stress and Inflammation Caused by Cisplatin OtotoxicityDocumento14 páginasAntioxidants: Oxidative Stress and Inflammation Caused by Cisplatin OtotoxicityWahyu Dwi NugrohoAinda não há avaliações
- How To Get Published in Top Journals - A Journey With EnagoDocumento24 páginasHow To Get Published in Top Journals - A Journey With EnagoWahyu Dwi NugrohoAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Effects Atra On Mmp-9 Activity and Integrin Expression in Choriocarcinoma Culture Cell Line Bewo (Atcc Ccl-98) First AuthorDocumento1 páginaEffects Atra On Mmp-9 Activity and Integrin Expression in Choriocarcinoma Culture Cell Line Bewo (Atcc Ccl-98) First AuthorWahyu Dwi NugrohoAinda não há avaliações
- ATLS Practice Test 1: Other ThanDocumento11 páginasATLS Practice Test 1: Other ThanGarcia Rosa75% (8)
- Atls MCQDocumento10 páginasAtls MCQTerri Sandi Susyanto67% (15)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- ATLS Practice Test 1: Other ThanDocumento11 páginasATLS Practice Test 1: Other ThanGarcia Rosa75% (8)
- ATLS Practice Test 1: Other ThanDocumento11 páginasATLS Practice Test 1: Other ThanGarcia Rosa75% (8)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Atls MCQDocumento10 páginasAtls MCQTerri Sandi Susyanto67% (15)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- ATLS Practice Test 1: Other ThanDocumento11 páginasATLS Practice Test 1: Other ThanGarcia Rosa75% (8)
- ATLS Practice Test 1: Other ThanDocumento11 páginasATLS Practice Test 1: Other ThanGarcia Rosa75% (8)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- ATLS Chapter Review QuestionsDocumento36 páginasATLS Chapter Review QuestionsKen Evans89% (57)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- ATLS Case ScenarioDocumento13 páginasATLS Case ScenarioJenny Schneider100% (2)
- Garda 17Documento45 páginasGarda 17Wahyu Dwi NugrohoAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Atls Summary ExaminationDocumento14 páginasAtls Summary Examinationelnikety100% (2)
- 6.diabetes Education in ChilDocumento9 páginas6.diabetes Education in ChilWahyu Dwi NugrohoAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- ATLSPracticeTest3 PDFDocumento10 páginasATLSPracticeTest3 PDFRodrigo Sanjines75% (4)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Analisis Bank-1Documento1 páginaAnalisis Bank-1Wahyu Dwi NugrohoAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- ATLS Practice Test 1: Other ThanDocumento11 páginasATLS Practice Test 1: Other ThanGarcia Rosa75% (8)
- Garda 17Documento45 páginasGarda 17Wahyu Dwi NugrohoAinda não há avaliações
- Aplastic Anemia - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFDocumento21 páginasAplastic Anemia - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFWahyu Dwi NugrohoAinda não há avaliações
- Garda 17Documento45 páginasGarda 17Wahyu Dwi NugrohoAinda não há avaliações
- Garda 17Documento45 páginasGarda 17Wahyu Dwi NugrohoAinda não há avaliações
- Garda 17Documento45 páginasGarda 17Wahyu Dwi NugrohoAinda não há avaliações
- Aplastic Anemia - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFDocumento21 páginasAplastic Anemia - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFWahyu Dwi NugrohoAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- UTI in DM - Super PaperDocumento6 páginasUTI in DM - Super PaperLourdes Fernandez CabreraAinda não há avaliações
- Lymposite MaturationDocumento1 páginaLymposite MaturationWahyu Dwi NugrohoAinda não há avaliações
- Quiz - Hemodynamic Disorders, Thromboembolic DiseaDocumento48 páginasQuiz - Hemodynamic Disorders, Thromboembolic DiseaAdrian CaballesAinda não há avaliações
- Emergency Medicine 1st Edition - DR - Waleed (101 Papers)Documento101 páginasEmergency Medicine 1st Edition - DR - Waleed (101 Papers)Mokhtar Moh100% (1)
- 250 سؤالDocumento57 páginas250 سؤالعلاء العاوور100% (4)
- Ecografia Toracica PDFDocumento12 páginasEcografia Toracica PDFCristinaLucanAinda não há avaliações
- PGY Duty Round整合版pdf 2020 v2Documento134 páginasPGY Duty Round整合版pdf 2020 v2Jacky 許智凱Ainda não há avaliações
- First Aid and Fire FightingDocumento29 páginasFirst Aid and Fire FightingMaissam MustafaAinda não há avaliações
- Citrate Protocol 2020Documento5 páginasCitrate Protocol 2020Katrina Mae AntalanAinda não há avaliações
- Chapter+04 9th+edition ITLS 04-2020Documento25 páginasChapter+04 9th+edition ITLS 04-2020Brhanemeskel MekonnenAinda não há avaliações
- GROUP 3 - CASE STUDY - TraumaDocumento5 páginasGROUP 3 - CASE STUDY - TraumaDinarkram Rabreca EculAinda não há avaliações
- Drug Study Threatened AbortionDocumento4 páginasDrug Study Threatened AbortionKath CastilloAinda não há avaliações
- English Mock MCDocumento9 páginasEnglish Mock MCapi-19867499Ainda não há avaliações
- Sepsis and SIRSDocumento22 páginasSepsis and SIRSDr.Deb Sanjay Nag100% (1)
- First AidDocumento39 páginasFirst Aidamila_vithanage100% (1)
- Approach To Acutely Ill PatientDocumento22 páginasApproach To Acutely Ill PatientSarah RamliAinda não há avaliações
- Burns in Small Animals - WSAVA2013 - VINDocumento4 páginasBurns in Small Animals - WSAVA2013 - VINApra ShahiAinda não há avaliações
- Management of Septic Shock in An Intermediate Care UnitDocumento20 páginasManagement of Septic Shock in An Intermediate Care UnitJHAinda não há avaliações
- EMD Guidecards PDFDocumento49 páginasEMD Guidecards PDFЛизатро1980 ЛизаAinda não há avaliações
- Final Ottawa Handbook of Emergency Medicine 4th Edition V4Documento63 páginasFinal Ottawa Handbook of Emergency Medicine 4th Edition V4Mohammed Alshamsi100% (4)
- Cardiogenic ShockDocumento8 páginasCardiogenic ShockMAE RACHELLE LAMOSTEAinda não há avaliações
- Canada Gateway MCC Qe Questions 1Documento100 páginasCanada Gateway MCC Qe Questions 1Kak KfgaAinda não há avaliações
- 71Documento27 páginas71onuchukwu chibuzorAinda não há avaliações
- Master Thesis DentistryDocumento5 páginasMaster Thesis Dentistrygbxwghwb100% (2)
- Case Study On GynaeDocumento22 páginasCase Study On GynaeJay PaulAinda não há avaliações
- Contemporary Perioperative Haemodynamic MonitoringDocumento12 páginasContemporary Perioperative Haemodynamic MonitoringrjerezrAinda não há avaliações
- 41 - Type of Shock PDFDocumento2 páginas41 - Type of Shock PDFjamesAinda não há avaliações
- Fiji Leptospirosis Clinical Guidelines - 10JUN - FINALDocumento25 páginasFiji Leptospirosis Clinical Guidelines - 10JUN - FINALAshviniAinda não há avaliações
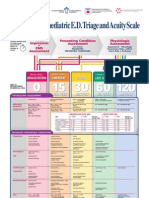
- Paediatric Triage PosterDocumento1 páginaPaediatric Triage PosterGenaro Olmos Garcia100% (2)
- Advanced Trauma Life SupportDocumento452 páginasAdvanced Trauma Life Supportnatalia100% (7)
- First Responder NotesDocumento8 páginasFirst Responder Notesjoe_a_salvatoreAinda não há avaliações
- 17 Protective Measures OKDocumento69 páginas17 Protective Measures OKMary Rose LatorreAinda não há avaliações
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (24)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)