Você também pode gostar
- Manajemen NyeriDocumento30 páginasManajemen NyeriEL SHITAAinda não há avaliações
- Manajemen NyeriDocumento33 páginasManajemen NyeriEL SHITAAinda não há avaliações
- Menu Meeting Package Up-Date 2018Documento4 páginasMenu Meeting Package Up-Date 2018EL SHITAAinda não há avaliações
- International Recruitment Application Form (New)Documento5 páginasInternational Recruitment Application Form (New)EL SHITAAinda não há avaliações
- Cardiac Ultrasound Echocardiography Made Easy Step-By-Step GuideDocumento1 páginaCardiac Ultrasound Echocardiography Made Easy Step-By-Step GuideEL SHITAAinda não há avaliações
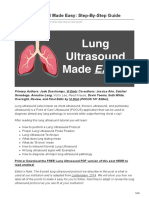
- Lung Ultrasound Made Easy Step-By-Step GuideDocumento48 páginasLung Ultrasound Made Easy Step-By-Step GuideEL SHITA100% (1)
- DVT Ultrasound Made Easy Step-By-Step GuideDocumento37 páginasDVT Ultrasound Made Easy Step-By-Step GuideEL SHITAAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Criminal Law 2 - Assignment 4-9 PDFDocumento4 páginasCriminal Law 2 - Assignment 4-9 PDFDaf MarianoAinda não há avaliações
- List SDGDocumento5 páginasList SDGsachinAinda não há avaliações
- LGR Curriculum v5-Final-B PDFDocumento83 páginasLGR Curriculum v5-Final-B PDFAfrian IndrawanAinda não há avaliações
- Ad Hoc International TribunalsDocumento6 páginasAd Hoc International TribunalsEnock ChengulaAinda não há avaliações
- Wa0006.Documento7 páginasWa0006.Anjana AjayAinda não há avaliações
- Gender Glossary of Terms and ConceptsDocumento17 páginasGender Glossary of Terms and ConceptsApril Jean BantaAinda não há avaliações
- Mega Moot PetitionerDocumento5 páginasMega Moot PetitionerSwaathi100% (2)
- Gender Equality in The WorkplaceDocumento3 páginasGender Equality in The WorkplaceRnyle RafaelAinda não há avaliações
- Full List of RecipientsDocumento28 páginasFull List of RecipientsLive 5 NewsAinda não há avaliações
- Commonwealth Human Rights InitiativeDocumento1 páginaCommonwealth Human Rights Initiativemyjoyonline.comAinda não há avaliações
- MCQ Questions CH-2Documento4 páginasMCQ Questions CH-2SANDHYA KUMARIAinda não há avaliações
- (U) Daily Activity Report: Marshall DistrictDocumento5 páginas(U) Daily Activity Report: Marshall DistrictFauquier NowAinda não há avaliações
- 2009 Caribbean Studies P1Documento13 páginas2009 Caribbean Studies P1Darrion BruceAinda não há avaliações
- Intersecting Violences: A Review of Feminist Theories and Debates On VAWG and Poverty in Latin AmericaDocumento70 páginasIntersecting Violences: A Review of Feminist Theories and Debates On VAWG and Poverty in Latin AmericaCAWNetworkAinda não há avaliações
- Dr. Craig Childress Professional LetterDocumento4 páginasDr. Craig Childress Professional Letterko_andrew9963Ainda não há avaliações
- Grade 9 Long Quiz 4TH QUARTERDocumento6 páginasGrade 9 Long Quiz 4TH QUARTERjameroprincess003Ainda não há avaliações
- The Philippines Data Privacy ActDocumento15 páginasThe Philippines Data Privacy ActMandala MimaropaAinda não há avaliações
- Naima Niambi - COPY: PASTE "FOR IMMEDIATE RELEASE: May 24, PDFDocumento3 páginasNaima Niambi - COPY: PASTE "FOR IMMEDIATE RELEASE: May 24, PDFBenjamin A Boyce100% (1)
- GEnder Studies Notes MergedDocumento81 páginasGEnder Studies Notes MergedKhadija AftabAinda não há avaliações
- Balancing Freedom of Expression and Hate Speech Ca PDFDocumento12 páginasBalancing Freedom of Expression and Hate Speech Ca PDFsheikh hialAinda não há avaliações
- Forum Script's About Child Abuse: Thank You, That 'S All From MeDocumento7 páginasForum Script's About Child Abuse: Thank You, That 'S All From Mehazalia othmanAinda não há avaliações
- Department of Education: Program ProposalDocumento21 páginasDepartment of Education: Program Proposalimelda d. lampaAinda não há avaliações
- CESCDocumento5 páginasCESCJohn Lennard CostunaAinda não há avaliações
- Addictive Disorder Diagnosis - EditedDocumento6 páginasAddictive Disorder Diagnosis - EditedANDREWAinda não há avaliações
- Multiple ChoiceDocumento23 páginasMultiple ChoiceCedrick OcampoAinda não há avaliações
- BJMPDocumento7 páginasBJMPMangampo Albert P.Ainda não há avaliações
- Julian Garcia - Quarter One EssayDocumento2 páginasJulian Garcia - Quarter One Essayapi-547354695Ainda não há avaliações
- Brainstorming 15 TopicsDocumento25 páginasBrainstorming 15 Topicsanhthu2005.tcAinda não há avaliações
- Sociology AssignmentDocumento6 páginasSociology AssignmentSWYAM MEHROTRAAinda não há avaliações
- Lesson III Claim Counterclaim RebuttalDocumento42 páginasLesson III Claim Counterclaim RebuttalBrian Angelo BernardoAinda não há avaliações