Você também pode gostar
- Case Study Presentation: "Ectopic Pregnancy"Documento8 páginasCase Study Presentation: "Ectopic Pregnancy"Sherwina Alih-BieberAinda não há avaliações
- The Importance of Dignity in All WorkDocumento2 páginasThe Importance of Dignity in All WorkFarhan AliAinda não há avaliações
- Ethical Principles of Paternalism in NursingDocumento10 páginasEthical Principles of Paternalism in NursingGladz C CadaguitAinda não há avaliações
- Persuasive Essay on Abortion RightsDocumento5 páginasPersuasive Essay on Abortion RightsgdeycazaAinda não há avaliações
- Post Partum Depression Final Presentation 2Documento7 páginasPost Partum Depression Final Presentation 2api-506871797100% (1)
- Normal Vaginal Delivery StepsDocumento6 páginasNormal Vaginal Delivery StepsT helper CellsAinda não há avaliações
- Mabini Colleges' Mission and Vision for Transforming StudentsDocumento12 páginasMabini Colleges' Mission and Vision for Transforming StudentsKaren Kate AblesAinda não há avaliações
- Causes, Symptoms & Risks of Ectopic PregnancyDocumento18 páginasCauses, Symptoms & Risks of Ectopic PregnancyMc_Lopez_1761Ainda não há avaliações
- Ectopic PregnancyDocumento33 páginasEctopic Pregnancyjedi006100% (1)
- WorksheetDocumento1 páginaWorksheetDarren CariñoAinda não há avaliações
- Ectopic Pregnancy Case StudyDocumento69 páginasEctopic Pregnancy Case StudyMo-nhica Luise AlundayAinda não há avaliações
- Cerebral Contusions and LacerationDocumento5 páginasCerebral Contusions and LacerationVithaa'TetaaAinda não há avaliações
- Post Partum DepressionDocumento9 páginasPost Partum DepressionNaufal BinseffAinda não há avaliações
- Amniotic Fluid EmbolismDocumento34 páginasAmniotic Fluid EmbolismReygie MataAinda não há avaliações
- School Timetable and RulesDocumento3 páginasSchool Timetable and Rulesmaydoni100% (2)
- Ectopic Pregnancy1Documento34 páginasEctopic Pregnancy1Kreshimaricon FurigayAinda não há avaliações
- Davao Doctors College Nursing Program Progress NotesDocumento17 páginasDavao Doctors College Nursing Program Progress NotesABBEYGALE JOYHN GALANAinda não há avaliações
- Case Study-Molar PregnancyDocumento14 páginasCase Study-Molar Pregnancysimbarashe tangwadzana100% (1)
- Generalized Anxiety Disorders (GAD)Documento8 páginasGeneralized Anxiety Disorders (GAD)Deasy Arindi PutriAinda não há avaliações
- Module 3 A PresentationDocumento79 páginasModule 3 A PresentationJesus William Arizapana MamaniAinda não há avaliações
- Ectopic PregnancyDocumento3 páginasEctopic PregnancySiska FriedmanAinda não há avaliações
- Ectopic PregnancyDocumento46 páginasEctopic PregnancyNoegi AkasAinda não há avaliações
- Pa Tho Physiology of Ectopic Pregnancy PDFDocumento2 páginasPa Tho Physiology of Ectopic Pregnancy PDFbowki namoAinda não há avaliações
- EpiglottitisDocumento1 páginaEpiglottitisSandra GabasAinda não há avaliações
- Primay Health CareDocumento6 páginasPrimay Health Careمحمد عبدالهادي إسماعيلAinda não há avaliações
- Obg Icd-10 Pregnancy, Childbirth, PuerperiumDocumento11 páginasObg Icd-10 Pregnancy, Childbirth, PuerperiumarifianjuariAinda não há avaliações
- Risk Factors and Vulnerable Groups for Negative PregnancyDocumento2 páginasRisk Factors and Vulnerable Groups for Negative PregnancyTechnoShindoAinda não há avaliações
- Rare Kidney Cancer in ChildrenDocumento12 páginasRare Kidney Cancer in ChildrenKath CamachoAinda não há avaliações
- 2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFDocumento4 páginas2.11 SEPTIC ABORTION AND SEPTIC SHOCK. M. Botes PDFteteh_thikeuAinda não há avaliações
- Hydatidiform MoleDocumento17 páginasHydatidiform MoleRizzamwah Catague0% (1)
- Drugs For GUTDocumento11 páginasDrugs For GUTAyesha LiaqatAinda não há avaliações
- CLONIDINE HYDROCHLORIDE: Cardiovascular and Analgesic AgentDocumento2 páginasCLONIDINE HYDROCHLORIDE: Cardiovascular and Analgesic AgentDOni CorleoneAinda não há avaliações
- ThesisDocumento27 páginasThesisKelsey Anne ZabalaAinda não há avaliações
- Pyloric StenosisDocumento16 páginasPyloric StenosisHelen McClintockAinda não há avaliações
- GRP 20 Final Abscess Case StudyDocumento14 páginasGRP 20 Final Abscess Case StudyBorja, Kimberly GraceAinda não há avaliações
- Placenta Previa: Bleeding During PregnancyDocumento8 páginasPlacenta Previa: Bleeding During PregnancyBj DuquesaAinda não há avaliações
- Ulcerative ColitisDocumento7 páginasUlcerative ColitisShaira Anne Fuentes BaroniaAinda não há avaliações
- Sheehan Syndrom L. HaddockDocumento9 páginasSheehan Syndrom L. Haddockfreddyop72Ainda não há avaliações
- H MoleDocumento27 páginasH MoleAnjela Fae Jintalan Amador100% (1)
- Thesis AcknowledgementsDocumento1 páginaThesis AcknowledgementsSin Yee LingAinda não há avaliações
- ER to Discharge CourseDocumento3 páginasER to Discharge CourseAljon S. TemploAinda não há avaliações
- Lecture 2 Skpx2043Lec2 Skpx2043 PDFDocumento29 páginasLecture 2 Skpx2043Lec2 Skpx2043 PDFGaleev George Lajuti100% (1)
- Gastrointestinal TractDocumento13 páginasGastrointestinal TractLucasAinda não há avaliações
- GBS Nursing MangementDocumento21 páginasGBS Nursing MangementJoseph Namita SunnyAinda não há avaliações
- Breast MassDocumento18 páginasBreast MassMishti Mokarrama100% (1)
- Placenta PreviaDocumento17 páginasPlacenta PreviaSundari AtmanegaraAinda não há avaliações
- PrednisoneDocumento3 páginasPrednisoneapi-3797941100% (1)
- A Reflection On Philippine PlanningDocumento3 páginasA Reflection On Philippine Planningar.ryanortigasAinda não há avaliações
- CRANIOTOMYDocumento31 páginasCRANIOTOMYDrVarun KaliaAinda não há avaliações
- Ectopic Pregnancy Diagnosis and TreatmentDocumento44 páginasEctopic Pregnancy Diagnosis and Treatment林昌恩Ainda não há avaliações
- Grabe Ka FinalDocumento57 páginasGrabe Ka FinalJoanne Bernadette AguilarAinda não há avaliações
- Maternal/Ob Notes: A Person's Sexuality Encompasses The Complex Behaviors, Attitudes Emotions and Preferences That AreDocumento37 páginasMaternal/Ob Notes: A Person's Sexuality Encompasses The Complex Behaviors, Attitudes Emotions and Preferences That Aresabao kizuiteAinda não há avaliações
- DYSTROPHYDocumento15 páginasDYSTROPHYleeyan2wenty6Ainda não há avaliações
- Amniotic Fluid EmbolismDocumento22 páginasAmniotic Fluid EmbolismJay Marie GonzagaAinda não há avaliações
- Trig IdentitiesDocumento6 páginasTrig IdentitiesGrace ChenAinda não há avaliações
- Abortion - The Great Injustice: by H.P. Dunn (1978)Documento14 páginasAbortion - The Great Injustice: by H.P. Dunn (1978)cdcrossroaderAinda não há avaliações
- InvictusDocumento4 páginasInvictusMonica GhețăuAinda não há avaliações
- Ectopic Pregnancy: A Life-Threatening ConditionDocumento15 páginasEctopic Pregnancy: A Life-Threatening ConditionMary Grace de RamosAinda não há avaliações
- Ectopic PregnancyDocumento3 páginasEctopic PregnancyMary Anne Yap100% (1)
- Ectopic Pregnancy: Medlineplus TopicsDocumento9 páginasEctopic Pregnancy: Medlineplus TopicsJonathan BendecioAinda não há avaliações
- Asian Recipes - Dessert Delights (With I - Ho, CharlesDocumento154 páginasAsian Recipes - Dessert Delights (With I - Ho, CharlesVanessa Santos100% (4)
- Chicken and Rice: IngredientsDocumento1 páginaChicken and Rice: IngredientsVanessa SantosAinda não há avaliações
- A Spark of ExistenceDocumento16 páginasA Spark of ExistenceVanessa SantosAinda não há avaliações
- Philippine Constitution PDFDocumento53 páginasPhilippine Constitution PDFVanessa SantosAinda não há avaliações
- Ps Calc GuideDocumento30 páginasPs Calc GuideMzee321Ainda não há avaliações
- Common Communicable DiseasesDocumento213 páginasCommon Communicable Diseasesɹǝʍdןnos100% (24)
- Personality Drawing TestDocumento1 páginaPersonality Drawing TestVanessa SantosAinda não há avaliações
- Chicken Mole EnchiladasDocumento2 páginasChicken Mole EnchiladasVanessa SantosAinda não há avaliações
- Critical Care Calculations Study GuideDocumento6 páginasCritical Care Calculations Study GuideAja Blue100% (2)
- Y Study CalculusDocumento5 páginasY Study CalculusVanessa SantosAinda não há avaliações
- Copar Final3Documento4 páginasCopar Final3Vanessa SantosAinda não há avaliações
- Marble speed needed to loop without fallingDocumento1 páginaMarble speed needed to loop without fallingVanessa SantosAinda não há avaliações
- Characteristics of Greek LiteratureDocumento2 páginasCharacteristics of Greek LiteratureVanessa Santos100% (2)
- Personality Drawing TestDocumento1 páginaPersonality Drawing TestVanessa SantosAinda não há avaliações
- The CourtDocumento6 páginasThe CourtVanessa SantosAinda não há avaliações
- Acute Abdominal Pain and Acute AppendicitisDocumento8 páginasAcute Abdominal Pain and Acute AppendicitisdrtpkAinda não há avaliações
- IMCIDocumento57 páginasIMCIwyndzAinda não há avaliações
- Republic Act No 9173Documento5 páginasRepublic Act No 9173Vanessa SantosAinda não há avaliações
- Shock Case Presentation: General DataDocumento1 páginaShock Case Presentation: General DataVanessa SantosAinda não há avaliações
- LymphomaDocumento15 páginasLymphomaVanessa SantosAinda não há avaliações
- FractureDocumento58 páginasFractureVanessa SantosAinda não há avaliações
- 40 Items Comprehensive NCLEX ReviewDocumento20 páginas40 Items Comprehensive NCLEX Reviewclumsy16Ainda não há avaliações
- Adrenergic ReceptorsDocumento6 páginasAdrenergic ReceptorsVanessa SantosAinda não há avaliações
- Spinal Disc HerniationDocumento12 páginasSpinal Disc HerniationVanessa SantosAinda não há avaliações
- Stone LowOxalateDiet PDFDocumento7 páginasStone LowOxalateDiet PDFVanessa Santos0% (1)
- CDPDocumento9 páginasCDPVanessa SantosAinda não há avaliações
- GreekDocumento7 páginasGreekVanessa SantosAinda não há avaliações
- IMCIDocumento57 páginasIMCIwyndzAinda não há avaliações
- AgingDocumento9 páginasAgingVanessa SantosAinda não há avaliações
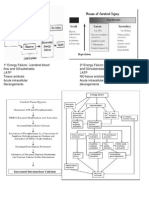
- 1º Energy FailureDocumento1 página1º Energy FailureVanessa SantosAinda não há avaliações
- Mole Concept - DPP 09 (Of Lec 13) - Yakeen 2.0 2024 (Legend)Documento3 páginasMole Concept - DPP 09 (Of Lec 13) - Yakeen 2.0 2024 (Legend)Romeshchandra Class X-CAinda não há avaliações
- Guidelines 2.0Documento4 páginasGuidelines 2.0Hansel TayongAinda não há avaliações
- R4 User GuideDocumento48 páginasR4 User GuideAaron SmithAinda não há avaliações
- Brooks Cole Empowerment Series Becoming An Effective Policy Advocate 7Th Edition Jansson Solutions Manual Full Chapter PDFDocumento36 páginasBrooks Cole Empowerment Series Becoming An Effective Policy Advocate 7Th Edition Jansson Solutions Manual Full Chapter PDFlois.guzman538100% (12)
- Levels of Attainment.Documento6 páginasLevels of Attainment.rajeshbarasaraAinda não há avaliações
- The Impact of Information Technology and Innovation To Improve Business Performance Through Marketing Capabilities in Online Businesses by Young GenerationsDocumento10 páginasThe Impact of Information Technology and Innovation To Improve Business Performance Through Marketing Capabilities in Online Businesses by Young GenerationsLanta KhairunisaAinda não há avaliações
- Youth, Time and Social Movements ExploredDocumento10 páginasYouth, Time and Social Movements Exploredviva_bourdieu100% (1)
- AIATS 2021 (OYMCF) Test 01 Offline - Code A - SolutionsDocumento34 páginasAIATS 2021 (OYMCF) Test 01 Offline - Code A - Solutionsbhavyakavya mehta100% (1)
- National Products Classification Code For Services in IndiaDocumento92 páginasNational Products Classification Code For Services in Indiakalanemi0% (2)
- The Emperor Jones: What's Inside in ContextDocumento27 páginasThe Emperor Jones: What's Inside in ContextHarshvardhan RaiAinda não há avaliações
- Rubric - Argumentative EssayDocumento2 páginasRubric - Argumentative EssayBobAinda não há avaliações
- Useful Coaching Questions: Questions To Create A State Change Questions To Ask When Something Goes WrongDocumento2 páginasUseful Coaching Questions: Questions To Create A State Change Questions To Ask When Something Goes WrongAntonioAinda não há avaliações
- BỘ GIÁO DỤC VÀ ĐÀO TẠO ĐỀ THI HỌC PHẦN KINH TẾ VĨ MÔDocumento5 páginasBỘ GIÁO DỤC VÀ ĐÀO TẠO ĐỀ THI HỌC PHẦN KINH TẾ VĨ MÔPhạm Thu NgaAinda não há avaliações
- Android Attendance Management SystemDocumento54 páginasAndroid Attendance Management Systemskpetks75% (12)
- Wsi PSDDocumento18 páginasWsi PSDДрагиша Небитни ТрифуновићAinda não há avaliações
- IEC-60721-3-3-2019 (Enviromental Conditions)Documento12 páginasIEC-60721-3-3-2019 (Enviromental Conditions)Electrical DistributionAinda não há avaliações
- CHB 2Documento15 páginasCHB 2Dr. Guruprasad Yashwant GadgilAinda não há avaliações
- Strain Gauge Sensor PDFDocumento12 páginasStrain Gauge Sensor PDFMario Eduardo Santos MartinsAinda não há avaliações
- The Slave Trade and The British Empire An Audit of Commemoration in WalesDocumento133 páginasThe Slave Trade and The British Empire An Audit of Commemoration in WaleslegoarkeologAinda não há avaliações
- Conserve O Gram: Understanding Histograms For Digital PhotographyDocumento4 páginasConserve O Gram: Understanding Histograms For Digital PhotographyErden SizgekAinda não há avaliações
- Policies and Regulations On EV Charging in India PPT KrishnaDocumento9 páginasPolicies and Regulations On EV Charging in India PPT KrishnaSonal ChoudharyAinda não há avaliações
- Manju Philip CVDocumento2 páginasManju Philip CVManju PhilipAinda não há avaliações
- Masonry Brickwork 230 MMDocumento1 páginaMasonry Brickwork 230 MMrohanAinda não há avaliações
- Moderntheater 170210003221 PDFDocumento80 páginasModerntheater 170210003221 PDFDycan MikeAinda não há avaliações
- PGP TutorialDocumento21 páginasPGP TutorialSabri AllaniAinda não há avaliações
- Startups Helping - India Go GreenDocumento13 páginasStartups Helping - India Go Greensimran kAinda não há avaliações
- Euro4 vehicle diesel engines 199 - 397 kW (270 - 540 hpDocumento6 páginasEuro4 vehicle diesel engines 199 - 397 kW (270 - 540 hpBranislava Savic63% (16)
- DAT MAPEH 6 Final PDFDocumento4 páginasDAT MAPEH 6 Final PDFMARLYN GAY EPANAinda não há avaliações
- Khaton Prayer BookDocumento47 páginasKhaton Prayer BookKarma TsheringAinda não há avaliações