Você também pode gostar
- Total Body HIIT Workout at HomeDocumento15 páginasTotal Body HIIT Workout at HomeLucia Milagros Perea VillacrezAinda não há avaliações
- Kinesiology Motion StudyDocumento7 páginasKinesiology Motion StudyEternal Inversionist100% (2)
- Lower Extremity (Special Tests) (FINAL)Documento7 páginasLower Extremity (Special Tests) (FINAL)Aubrey Vale SagunAinda não há avaliações
- Review Ortho Exam Lumbar Spine and Hip ConditionsDocumento11 páginasReview Ortho Exam Lumbar Spine and Hip ConditionsErin Hoffmann100% (3)
- Gluteal Muscle Activation During Common Therapeutic ExercisesDocumento17 páginasGluteal Muscle Activation During Common Therapeutic ExercisesJorge Lucas JimenezAinda não há avaliações
- Knee ExaminationDocumento14 páginasKnee ExaminationAsimAinda não há avaliações
- Differential Diagnosis MSK PathoDocumento13 páginasDifferential Diagnosis MSK PatholizAinda não há avaliações
- Yoga For Neck and Shoulder Paine BookDocumento13 páginasYoga For Neck and Shoulder Paine BookRu RuAinda não há avaliações
- Men's Health PDFDocumento100 páginasMen's Health PDFRkarwal Karwal100% (3)
- Differentials and Tests Condition Condition: TH THDocumento4 páginasDifferentials and Tests Condition Condition: TH THlawlor_jcAinda não há avaliações
- Clinical Signs - NamedDocumento9 páginasClinical Signs - NamedsprapurAinda não há avaliações
- Differential Diagnosis of Back PainDocumento26 páginasDifferential Diagnosis of Back PainKristy Besarab100% (1)
- Upper and Lower Limb Clinical Notes (Snell)Documento12 páginasUpper and Lower Limb Clinical Notes (Snell)Martin Clyde100% (1)
- Orthopedics PDFDocumento193 páginasOrthopedics PDFJulie Anne CalusimAinda não há avaliações
- Muscles of the Head, Neck, and TrunkDocumento8 páginasMuscles of the Head, Neck, and TrunkJericho CarenaAinda não há avaliações
- Applied KinesiologyDocumento8 páginasApplied KinesiologyJose Luis25% (8)
- Meralgia ParestheticaaDocumento28 páginasMeralgia ParestheticaaShabana AfzalAinda não há avaliações
- Subtle Body Kriya For Refinement Kundalini YogaDocumento4 páginasSubtle Body Kriya For Refinement Kundalini Yogatimsmith1081574Ainda não há avaliações
- Katya 30-Day-Challenge-Bikini-Body-Week-1 PDFDocumento8 páginasKatya 30-Day-Challenge-Bikini-Body-Week-1 PDFGeraldyneAinda não há avaliações
- Facilitated Positional Release FPRDocumento12 páginasFacilitated Positional Release FPRcoahuiltecoAinda não há avaliações
- Alterations in Locomotion Concept Map - NC3.drawioDocumento16 páginasAlterations in Locomotion Concept Map - NC3.drawioCARLOS JOSETON PAOLO SANTIAGO TORREAinda não há avaliações
- POTT: Concise Title for Hip Muscle TestsDocumento4 páginasPOTT: Concise Title for Hip Muscle TestsDesi SmithAinda não há avaliações
- Case 2: Ask The Questions About What Pain Activity Causes The Pain?Documento8 páginasCase 2: Ask The Questions About What Pain Activity Causes The Pain?api-479717740Ainda não há avaliações
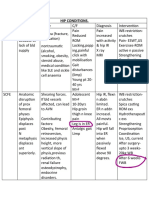
- HIP CONDITIONS GUIDEDocumento2 páginasHIP CONDITIONS GUIDEseemaAinda não há avaliações
- LBP QualifDocumento37 páginasLBP Qualifchaer assofiAinda não há avaliações
- Caporusso Ankle Arthrodesis Rehab ProtocolDocumento1 páginaCaporusso Ankle Arthrodesis Rehab ProtocolGonzalo QuiñonesAinda não há avaliações
- Week 9 - PCPDocumento7 páginasWeek 9 - PCPapi-479754549Ainda não há avaliações
- Anamnesis: Inspeksi: Palpasi:: Pasien Dengan Low Back PainDocumento3 páginasAnamnesis: Inspeksi: Palpasi:: Pasien Dengan Low Back PainRanggah RajasaAinda não há avaliações
- MSK Important TablesDocumento3 páginasMSK Important TablesnikitaybhavsarAinda não há avaliações
- Lower Back Pain Diagnostic AlgorithmDocumento1 páginaLower Back Pain Diagnostic AlgorithmZia HaywoodAinda não há avaliações
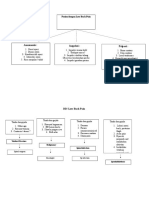
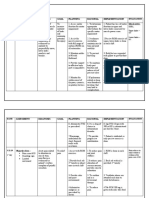
- Nursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataDocumento8 páginasNursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataMoonAinda não há avaliações
- LowBackPainDocumento3 páginasLowBackPainFATHICHAHAinda não há avaliações
- Hip and Lumbar Spine Physical Exam FindingsDocumento11 páginasHip and Lumbar Spine Physical Exam FindingsRiaAinda não há avaliações
- Ankle & Lower Leg SummaryDocumento11 páginasAnkle & Lower Leg SummaryAnnelieAinda não há avaliações
- ORTHOPAEDICS MANUAL PaulDocumento62 páginasORTHOPAEDICS MANUAL PaulRAinda não há avaliações
- Hip Disorders SummaryDocumento2 páginasHip Disorders SummarybhnsboshkashAinda não há avaliações
- Exercise 1 Differential Chart: Ddx-Hip Region of Pain Risk Factors Aggravating/Relieving Treatment OsteoarthritisDocumento2 páginasExercise 1 Differential Chart: Ddx-Hip Region of Pain Risk Factors Aggravating/Relieving Treatment Osteoarthritisapi-479720222Ainda não há avaliações
- Week 10 - PCPDocumento3 páginasWeek 10 - PCPapi-479754549Ainda não há avaliações
- Femoral Anterior Glide SyndromeDocumento25 páginasFemoral Anterior Glide SyndromeMartinKozjanAinda não há avaliações
- Exercise 1 Differential ChartDocumento6 páginasExercise 1 Differential Chartapi-479717740Ainda não há avaliações
- Posterior, Lateral, and Anterior Hip Pain Due To Musculoskeletal OriginDocumento4 páginasPosterior, Lateral, and Anterior Hip Pain Due To Musculoskeletal Origin楊畯凱Ainda não há avaliações
- Athlete EffectsDocumento3 páginasAthlete Effectscoach.mcgill12Ainda não há avaliações
- Ankle Practical CRFDocumento8 páginasAnkle Practical CRFapi-640939939Ainda não há avaliações
- Exercise 1Documento4 páginasExercise 1api-479754549Ainda não há avaliações
- wk-10 pcp1 Study Guide Ques-AnsDocumento8 páginaswk-10 pcp1 Study Guide Ques-Ansapi-453771787Ainda não há avaliações
- Pemeriksaan Fisik Tulang BelakangDocumento35 páginasPemeriksaan Fisik Tulang BelakangLeaf CloverAinda não há avaliações
- Pathway For Shoulder PainDocumento1 páginaPathway For Shoulder Painrizk86Ainda não há avaliações
- Mus Culo SkeletalDocumento7 páginasMus Culo SkeletalJessica Abella SohAinda não há avaliações
- Week 10 PCP Workbook QuestionsDocumento6 páginasWeek 10 PCP Workbook Questionsapi-479717740Ainda não há avaliações
- Exams To Confirm and Negate Spinal Spondy and StenoDocumento5 páginasExams To Confirm and Negate Spinal Spondy and StenoKSAinda não há avaliações
- Neurological ObservationsDocumento2 páginasNeurological Observationsevripidis tziokasAinda não há avaliações
- Comparison of Rheumatoid and OsteoarthritisDocumento4 páginasComparison of Rheumatoid and OsteoarthritisWaseem Khan AfridiAinda não há avaliações
- InjuriesDocumento60 páginasInjuriesIkkeNur AnindytaaAinda não há avaliações
- 3.1 Cervical Spine & TMJDocumento5 páginas3.1 Cervical Spine & TMJAIREN MARGARET MAGDALENAAinda não há avaliações
- Shoulder Complex SummaryDocumento10 páginasShoulder Complex SummaryAnnelieAinda não há avaliações
- UseofMulliganSNAGs PDFDocumento1 páginaUseofMulliganSNAGs PDFMestereaga AlinAinda não há avaliações
- Physical Rehabilitation 2.2 Rehabilitation of Lower Limb Musculoskeletal DisordersDocumento6 páginasPhysical Rehabilitation 2.2 Rehabilitation of Lower Limb Musculoskeletal DisordersJAIRISH YZABELLE SALVADORAinda não há avaliações
- B15 M4 - Sports Injury (Dr. W. Mana-Ay 2014)Documento8 páginasB15 M4 - Sports Injury (Dr. W. Mana-Ay 2014)Dakila Vine VillanAinda não há avaliações
- Act. 2.1Documento2 páginasAct. 2.1mix shopAinda não há avaliações
- Hip Labrum and FAI Post-Surgical Rehabilitation GuidelineDocumento5 páginasHip Labrum and FAI Post-Surgical Rehabilitation GuidelineLéo ToaldoAinda não há avaliações
- Era University Era College of NursingDocumento8 páginasEra University Era College of NursingAru Verma100% (1)
- Non-Operative Hip Rehab GuideDocumento4 páginasNon-Operative Hip Rehab GuideBurr NerrAinda não há avaliações
- Lower Extremity Special TestsDocumento16 páginasLower Extremity Special TestsAlyssa BatasAinda não há avaliações
- Degenerative in ShoulderDocumento49 páginasDegenerative in Shoulderari rujatiAinda não há avaliações
- Arthritis GuideDocumento1 páginaArthritis GuideAlpacaAinda não há avaliações
- Jospt 1979 1 1 23Documento13 páginasJospt 1979 1 1 23pkrajniAinda não há avaliações
- Ini Al Evalua On/plan of Care - 6/27/2019: AssessmentDocumento2 páginasIni Al Evalua On/plan of Care - 6/27/2019: AssessmentlizAinda não há avaliações
- Upper and Lower Limbs Neurological Exam atfDocumento6 páginasUpper and Lower Limbs Neurological Exam atfmnahmed2000Ainda não há avaliações
- Grand PracsDocumento4 páginasGrand PracsChristian Allen SibalaAinda não há avaliações
- Tensegrity in Cadaveric StudyDocumento5 páginasTensegrity in Cadaveric StudyJohn SharkeyAinda não há avaliações
- Roblin HealyDocumento6 páginasRoblin HealyMiguel JohnsonAinda não há avaliações
- Orthopaedics DocumentDocumento131 páginasOrthopaedics DocumentRazvan NegritasAinda não há avaliações
- Major Joint Movements PE ProjectDocumento11 páginasMajor Joint Movements PE ProjectSujata GayenAinda não há avaliações
- Wajah: Dan PengunyohDocumento8 páginasWajah: Dan PengunyohRetno Noor FebbyAinda não há avaliações
- Using A Trevira TubeDocumento8 páginasUsing A Trevira TubebranislavAinda não há avaliações
- GFHDocumento34 páginasGFHaisa mutiaraAinda não há avaliações
- Adhesive CapsulitisDocumento40 páginasAdhesive CapsulitisZirco HereAinda não há avaliações
- JointsDocumento4 páginasJointsotaibynaifAinda não há avaliações
- Chap22-Shoulder ComplexDocumento50 páginasChap22-Shoulder ComplextjAinda não há avaliações
- Jenkins, 2010 PDFDocumento13 páginasJenkins, 2010 PDFPablo fernandezAinda não há avaliações
- Artrodese Punho - ReviewDocumento8 páginasArtrodese Punho - ReviewLeonardo RochaAinda não há avaliações
- Arch Strengthen ExDocumento3 páginasArch Strengthen ExSylvia GraceAinda não há avaliações
- Breast AnatomyDocumento2 páginasBreast Anatomysweetenmonica80Ainda não há avaliações
- Congenital Dislocation of The Knee - RP's Ortho NotesDocumento3 páginasCongenital Dislocation of The Knee - RP's Ortho NotesSabari NathAinda não há avaliações
- Complete Lower Body and Core Workout with LungesDocumento3 páginasComplete Lower Body and Core Workout with LungesSerifa PasovicAinda não há avaliações
- Treating Clavicle and Proximal Humerus FracturesDocumento47 páginasTreating Clavicle and Proximal Humerus FracturesLinda SugiartoAinda não há avaliações
- Flexor Tendon Repair, Rehabilitation, and Reconstruction: Preoperative AssessmentDocumento11 páginasFlexor Tendon Repair, Rehabilitation, and Reconstruction: Preoperative AssessmentAdRiaNa JuLIetH LoZaDa PaTiÑoAinda não há avaliações
- Splinting The FingersDocumento17 páginasSplinting The FingersValentinaRestrepoAinda não há avaliações