Você também pode gostar
- Outpatient Referral Guidelines: NeurosurgeryDocumento11 páginasOutpatient Referral Guidelines: NeurosurgeryYuvraj Chauhan100% (1)
- Total Knee Replacement - Patient Information BookletDocumento24 páginasTotal Knee Replacement - Patient Information BookletCotard Delusion100% (1)
- GANG FIT (Part 2)Documento58 páginasGANG FIT (Part 2)John WangAinda não há avaliações
- MEDSURG - Cellular AberrationDocumento10 páginasMEDSURG - Cellular AberrationLeslie CruzAinda não há avaliações
- Bupa Offer - EnglishDocumento1 páginaBupa Offer - EnglishAhmed Mohammed AIbrahimAinda não há avaliações
- Balsam Leaflet en PDFDocumento8 páginasBalsam Leaflet en PDFEng. Waleed AhmedAinda não há avaliações
- InsuranceDocumento6 páginasInsuranceIssam AzarAinda não há avaliações
- Brochure - EZCare (Nov 2022)Documento11 páginasBrochure - EZCare (Nov 2022)Darren ChenAinda não há avaliações
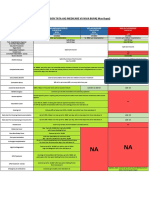
- Comparison Tata Aig Medicare Vs Niva BupaDocumento1 páginaComparison Tata Aig Medicare Vs Niva BupaTikekar ShubhamAinda não há avaliações
- Marsh PNG Local Medicare PlanDocumento1 páginaMarsh PNG Local Medicare PlanLeslie AtaemboAinda não há avaliações
- Insurance 20 - 21Documento3 páginasInsurance 20 - 21api-354358122Ainda não há avaliações
- Protect What You Treasure Most: HealthDocumento12 páginasProtect What You Treasure Most: HealthNelly HAinda não há avaliações
- Happy Family Floater - Policy NewDocumento45 páginasHappy Family Floater - Policy Newpooja singhalAinda não há avaliações
- GlobalCare Health Plan Benefits at a GlanceDocumento7 páginasGlobalCare Health Plan Benefits at a GlanceIrwanto AyongAinda não há avaliações
- Benefits Manual: Wipro Mediclaim InsuranceDocumento11 páginasBenefits Manual: Wipro Mediclaim InsuranceRavi TejaAinda não há avaliações
- Marsh PNG Local Medicare Plan: Details CommentaryDocumento1 páginaMarsh PNG Local Medicare Plan: Details CommentaryJoeAinda não há avaliações
- Supreme Health - 2021Documento2 páginasSupreme Health - 2021raeshawn1980Ainda não há avaliações
- Virtusa Policy Benefit1Documento1 páginaVirtusa Policy Benefit1Venkatesh KumarAinda não há avaliações
- Axa QuoteDocumento2 páginasAxa QuoteDanny OtAinda não há avaliações
- Daleel E PDFDocumento44 páginasDaleel E PDFNumair AshrafAinda não há avaliações
- Copy of 2020 ID List of Benefits and Allowances ARZxlsx - 2. Medical Insurance UpdDocumento1 páginaCopy of 2020 ID List of Benefits and Allowances ARZxlsx - 2. Medical Insurance Updfrututu.smoothiesAinda não há avaliações
- Healthy You One Pager - 21-04-20Documento2 páginasHealthy You One Pager - 21-04-20Anu PriyaAinda não há avaliações
- Individual Product - RatesTOB - V7Documento3 páginasIndividual Product - RatesTOB - V7Hanifa MohammedAinda não há avaliações
- Health & Dental Handout JUN17Documento2 páginasHealth & Dental Handout JUN17Darius YangAinda não há avaliações
- ReyForBusiness (Group) - Plan & Price Sampling - 2023Documento7 páginasReyForBusiness (Group) - Plan & Price Sampling - 2023Nadhifah Nur HafshahAinda não há avaliações
- Apollo Munich Health Insurance Co. Ltd. Products and PoliciesDocumento8 páginasApollo Munich Health Insurance Co. Ltd. Products and PoliciesNuha SamsAinda não há avaliações
- Apollo Munich Health Insurance CoDocumento8 páginasApollo Munich Health Insurance CoNuha SamsAinda não há avaliações
- Niva ReAssure SS v11Documento2 páginasNiva ReAssure SS v11CHELLASWAMY RAMASWAMYAinda não há avaliações
- v8 Comparison of A Ips - Sep 2022Documento4 páginasv8 Comparison of A Ips - Sep 2022Wenwei ChionhAinda não há avaliações
- ReAssure_SSDocumento2 páginasReAssure_SSAmit Kumar KandiAinda não há avaliações
- Member Certificate 70749421 1Documento2 páginasMember Certificate 70749421 1abadir.abdiAinda não há avaliações
- Comparison Quote - GPADocumento7 páginasComparison Quote - GPAvisheshAinda não há avaliações
- Niva PB ReAssure SS v5Documento2 páginasNiva PB ReAssure SS v5samdsozaAinda não há avaliações
- A-Plus Total Health BrochureDocumento2 páginasA-Plus Total Health BrochureAIA Sunnie YapAinda não há avaliações
- Reassurance at Every Step: Keeps Giving You More!Documento2 páginasReassurance at Every Step: Keeps Giving You More!ASHOK NAGESHWARANAinda não há avaliações
- COMPLETE HEALTH INSURANCE WITH COVID COVERAGEDocumento2 páginasCOMPLETE HEALTH INSURANCE WITH COVID COVERAGEPRADEEP GUPTAAinda não há avaliações
- Niva ReAssure SS v3Documento2 páginasNiva ReAssure SS v3Arun GoyalAinda não há avaliações
- Niva ReAssure SS v3Documento2 páginasNiva ReAssure SS v3megha mazumdarAinda não há avaliações
- Niva ReAssure SS v3Documento2 páginasNiva ReAssure SS v3arya aroraAinda não há avaliações
- Reassurance at Every Step: Keeps Giving You More!Documento2 páginasReassurance at Every Step: Keeps Giving You More!rajatshrimalAinda não há avaliações
- My Family Guidance N Providers Network enDocumento52 páginasMy Family Guidance N Providers Network ensyed jeelani ahmedAinda não há avaliações
- Proposal For Group Mediclaim Insurance Total Premium (Rs. Excluding GST) Total Premium (Rs. Including GST)Documento3 páginasProposal For Group Mediclaim Insurance Total Premium (Rs. Excluding GST) Total Premium (Rs. Including GST)rajts singhAinda não há avaliações
- UNITY GMC - RFQ With DataDocumento27 páginasUNITY GMC - RFQ With DataBOC ClaimsAinda não há avaliações
- Upul 15 Yrs PDFDocumento4 páginasUpul 15 Yrs PDFMadawa DasarathnaAinda não há avaliações
- DIC E Care Products 2021Documento2 páginasDIC E Care Products 2021Trency FernandesAinda não há avaliações
- Medical BenefitsDocumento18 páginasMedical BenefitsTerra AnomaliaeAinda não há avaliações
- Royal Sundaram General Insurance Co. Limited (Formerly Known As Royal Sundaram Alliance Insurance Company Limited)Documento2 páginasRoyal Sundaram General Insurance Co. Limited (Formerly Known As Royal Sundaram Alliance Insurance Company Limited)Abhijit MohantyAinda não há avaliações
- Bon ClassicDocumento12 páginasBon ClassicJonathan BorleyAinda não há avaliações
- 202301.01 TNC Zomato GMC (New Plan With Dependents) RenewalDocumento23 páginas202301.01 TNC Zomato GMC (New Plan With Dependents) Renewalajptl92Ainda não há avaliações
- Optima Restore Brochure 1Documento8 páginasOptima Restore Brochure 1abhi_1mehrotaAinda não há avaliações
- Comprehensive Summary of Bupa Health Insurance and Dental BenefitsDocumento2 páginasComprehensive Summary of Bupa Health Insurance and Dental BenefitsShirishAinda não há avaliações
- SOB - 01 Sep 2019 PDFDocumento9 páginasSOB - 01 Sep 2019 PDFJacky_LEOLEOAinda não há avaliações
- Travelsafe With COVID-19 Coverage - 2022-08 (August 15)Documento5 páginasTravelsafe With COVID-19 Coverage - 2022-08 (August 15)Kre GLAinda não há avaliações
- ProductsDocumento3 páginasProductsYaseenAinda não há avaliações
- HS 360 One PagerDocumento4 páginasHS 360 One PagerpratheepAinda não há avaliações
- Policy DockDocumento16 páginasPolicy DockBruceAinda não há avaliações
- Senior Citizens Red Carpet Health Insurance Policy PDFDocumento8 páginasSenior Citizens Red Carpet Health Insurance Policy PDFrohit22221Ainda não há avaliações
- Choice MVDocumento1 páginaChoice MVGowell SupportAinda não há avaliações
- Compare Silver and Gold Health Insurance Plans Under 40 CharactersDocumento4 páginasCompare Silver and Gold Health Insurance Plans Under 40 CharactersMitra LalAinda não há avaliações
- Young Star - One Pager - Version 1.2 - August 2021Documento1 páginaYoung Star - One Pager - Version 1.2 - August 2021Satya ArchangelAinda não há avaliações
- Clientèle H.E.L.P Plan pays up to R200K hospital expensesDocumento3 páginasClientèle H.E.L.P Plan pays up to R200K hospital expensesItumeleng TshepisoAinda não há avaliações
- Benefit at A GlanceDocumento2 páginasBenefit at A GlanceShiv ChauhanAinda não há avaliações
- Health Insurance - Variants: # Description Medisure Prime Medisure Classic Medisure PLUS Medisure Super Top UpDocumento1 páginaHealth Insurance - Variants: # Description Medisure Prime Medisure Classic Medisure PLUS Medisure Super Top UpRajarshi GuhaAinda não há avaliações
- Cc122 DynaDocumento1 páginaCc122 DynaCarlo Me0% (1)
- Rosenbour Kenworth Fighter Outline Drawing A05562Documento1 páginaRosenbour Kenworth Fighter Outline Drawing A05562Carlo MeAinda não há avaliações
- Crane of 3 Ton MeterDocumento1 páginaCrane of 3 Ton MeterCarlo MeAinda não há avaliações
- Crane 7 TonsDocumento1 páginaCrane 7 TonsCarlo MeAinda não há avaliações
- Crane of 3 Ton MeterDocumento1 páginaCrane of 3 Ton MeterCarlo MeAinda não há avaliações
- To Define Clinical Psychology, Here Is A Definition From American Psychological Association's Division 12Documento14 páginasTo Define Clinical Psychology, Here Is A Definition From American Psychological Association's Division 12Summer LoveAinda não há avaliações
- FP Rescue Plan TemplateDocumento7 páginasFP Rescue Plan TemplateEmrahAinda não há avaliações
- MortuaryDocumento6 páginasMortuaryDr.Rajesh KamathAinda não há avaliações
- 1a - Hernandez - Research PaperDocumento28 páginas1a - Hernandez - Research PaperEdgar TorresAinda não há avaliações
- FMTDocumento29 páginasFMTCynfully SweetAinda não há avaliações
- Understanding Literature SynthesisDocumento5 páginasUnderstanding Literature SynthesisJimboy MaglonAinda não há avaliações
- MR T Balakrishnan PDFDocumento19 páginasMR T Balakrishnan PDFvinnyAinda não há avaliações
- Hinkle 15 eDocumento29 páginasHinkle 15 eamaan danishAinda não há avaliações
- 326 Mental - Status - Examination Directions and RubricDocumento4 páginas326 Mental - Status - Examination Directions and Rubricmp1757Ainda não há avaliações
- Principles of Toxicology or A Small Dose of Toxicology: Introduction and HistoryDocumento22 páginasPrinciples of Toxicology or A Small Dose of Toxicology: Introduction and HistoryMarisol CGAinda não há avaliações
- Epifeed LHFDocumento2 páginasEpifeed LHFJoko WiwiAinda não há avaliações
- 18-294 - CDG CSD Hba1c (1 X 2 M) Pull-Up (Diastika) - Ind - PrintDocumento1 página18-294 - CDG CSD Hba1c (1 X 2 M) Pull-Up (Diastika) - Ind - PrintHinama ChenAinda não há avaliações
- MikmikDocumento2 páginasMikmikMaria Mikaela PelagioAinda não há avaliações
- Milrinone As Compared With DobutamineDocumento10 páginasMilrinone As Compared With DobutamineArquivos DiversosAinda não há avaliações
- M102 Notes 3. Presumptive Sign: Extreme Form of Morning Sickness ThatDocumento3 páginasM102 Notes 3. Presumptive Sign: Extreme Form of Morning Sickness ThatNano KaAinda não há avaliações
- Jayden Alexander Tirta - Speech PreparationDocumento5 páginasJayden Alexander Tirta - Speech PreparationJAYDEN ALEXANDER TIRTAAinda não há avaliações
- White Paper Drugdelivery Needles Need Less MinDocumento13 páginasWhite Paper Drugdelivery Needles Need Less MinAmit PaulAinda não há avaliações
- Akhil Kumar Ramesh Halpani: Organization Structure Training AT Sukraft Recycling PVT Ltd. (Satari, Goa)Documento35 páginasAkhil Kumar Ramesh Halpani: Organization Structure Training AT Sukraft Recycling PVT Ltd. (Satari, Goa)Akhil PatelAinda não há avaliações
- Vitamin D and CalciumDocumento33 páginasVitamin D and CalciumAkhmadRoziAinda não há avaliações
- PSW Weclome LetterDocumento5 páginasPSW Weclome LetterMallius AllerisAinda não há avaliações
- Transfusion Guideline JAMADocumento11 páginasTransfusion Guideline JAMAandus007Ainda não há avaliações
- hw320 Unit 9 Final Assigment Stacey StoryDocumento15 páginashw320 Unit 9 Final Assigment Stacey Storyapi-651674228Ainda não há avaliações
- New ? Environmental Protection Essay 2022 - Let's Save Our EnvironmentDocumento22 páginasNew ? Environmental Protection Essay 2022 - Let's Save Our EnvironmentTaba TaraAinda não há avaliações
- 768 - Edited by Yashwardhan Bansal - MEDICAL NEGLIGENCE AND MALPRACTICE A THREAT TO HUMANITY - Shivani UpadhyayDocumento12 páginas768 - Edited by Yashwardhan Bansal - MEDICAL NEGLIGENCE AND MALPRACTICE A THREAT TO HUMANITY - Shivani UpadhyayANDREW JOSEPHAinda não há avaliações
- 5150 Holds in San Diego CountyDocumento28 páginas5150 Holds in San Diego CountynoxinqwertyAinda não há avaliações
- PED011 Final Req 15Documento3 páginasPED011 Final Req 15macabalang.yd501Ainda não há avaliações