Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Astra Zeneca - D8110C00001 - CSP-v2Documento111 páginasAstra Zeneca - D8110C00001 - CSP-v2Urgente24Ainda não há avaliações
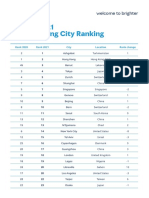
- GL 2021 Cost of Living City Ranking Mercer 0622Documento9 páginasGL 2021 Cost of Living City Ranking Mercer 0622Stathis MetsovitisAinda não há avaliações
- S&F Informe PBA Noviembre 2020.Documento20 páginasS&F Informe PBA Noviembre 2020.Urgente24Ainda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Lancet Advierte A Gobiernos y Asesores Porqué Ahora La Fase 4 Es Más Importante Que La Fase 3Documento3 páginasThe Lancet Advierte A Gobiernos y Asesores Porqué Ahora La Fase 4 Es Más Importante Que La Fase 3Urgente24Ainda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Blackrock - Indicative Debt Restructuring Terms and FrameworkDocumento1 páginaBlackrock - Indicative Debt Restructuring Terms and FrameworkUrgente24Ainda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Canal 9: Falló A Favor de Remigio Ángel González González en Un Litigio Contra El Abogado Carlos Lorefice LynchDocumento130 páginasCanal 9: Falló A Favor de Remigio Ángel González González en Un Litigio Contra El Abogado Carlos Lorefice LynchClaudio Andrés De LucaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- El Embargo A Robert BoschDocumento3 páginasEl Embargo A Robert BoschUrgente24Ainda não há avaliações
- Ganadores y Perdedores Según JP MorganDocumento10 páginasGanadores y Perdedores Según JP MorganUrgente24Ainda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- FCA Enters Into 6.3 Billion Credit Facility With Intesa SanpaoloDocumento3 páginasFCA Enters Into 6.3 Billion Credit Facility With Intesa SanpaoloUrgente24Ainda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Credit Suisse Sobre La Oferta de La ArgentinaDocumento3 páginasCredit Suisse Sobre La Oferta de La ArgentinaUrgente24Ainda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Informe Del Credit Suisse Sobre Oferta Argentina de DeudaDocumento6 páginasInforme Del Credit Suisse Sobre Oferta Argentina de DeudaUrgente24Ainda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Informe Jul19 NacionalDocumento30 páginasInforme Jul19 NacionalUrgente24Ainda não há avaliações
- Peace To ProsperityDocumento181 páginasPeace To ProsperityJoshua Davidovich100% (12)
- Encuesta Sobre La Satisfacción Con La DemocraciaDocumento34 páginasEncuesta Sobre La Satisfacción Con La DemocraciaUrgente24Ainda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Carta Intendentes A VidalDocumento5 páginasCarta Intendentes A VidalUrgente24Ainda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- 2020 World Watch ListDocumento68 páginas2020 World Watch ListtercerangelAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Importante Definición de Sergio MassaDocumento1 páginaImportante Definición de Sergio MassaUrgente24Ainda não há avaliações
- La Denuncia Del "Soplón"Documento9 páginasLa Denuncia Del "Soplón"Urgente24Ainda não há avaliações
- Unclassified Memorandum of Telephone ConversationDocumento5 páginasUnclassified Memorandum of Telephone ConversationThe Guardian91% (34)
- Reigniting Growth in Low-Income en Emerging Market - FMIDocumento28 páginasReigniting Growth in Low-Income en Emerging Market - FMIUrgente24Ainda não há avaliações
- Veeam CDM Report Infographic 2019 ES LATDocumento1 páginaVeeam CDM Report Infographic 2019 ES LATUrgente24Ainda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elypsis Political Outlook - Pole PositionDocumento7 páginasElypsis Political Outlook - Pole PositionUrgente24Ainda não há avaliações
- Syllabus Math 305Documento4 páginasSyllabus Math 305Nataly SusanaAinda não há avaliações
- Brain Alchemy Masterclass PsychotacticsDocumento87 páginasBrain Alchemy Masterclass Psychotacticskscmain83% (6)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- 11-Potential Use of Volcanic Pumice As A Construction Materialhossain2004Documento7 páginas11-Potential Use of Volcanic Pumice As A Construction Materialhossain2004afzal taiAinda não há avaliações
- Article On Role of Cyberspace in Geopolitics-PegasusDocumento5 páginasArticle On Role of Cyberspace in Geopolitics-PegasusIJRASETPublicationsAinda não há avaliações
- Analysis of Mozarts k.475Documento2 páginasAnalysis of Mozarts k.475ASPASIA FRAGKOUAinda não há avaliações
- Nanomedicine Lecture 2007Documento59 páginasNanomedicine Lecture 200778912071Ainda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Anzsco SearchDocumento6 páginasAnzsco SearchytytAinda não há avaliações
- ECDIS Presentation Library 4Documento16 páginasECDIS Presentation Library 4Orlando QuevedoAinda não há avaliações
- Esp-2000 BSDocumento6 páginasEsp-2000 BSByron LopezAinda não há avaliações
- InfltiDocumento13 páginasInfltiLEKH021Ainda não há avaliações
- PET Formal Letter SamplesDocumento7 páginasPET Formal Letter SamplesLe Anh ThuAinda não há avaliações
- What Are The Challenges and Opportunities of ResearchingDocumento5 páginasWhat Are The Challenges and Opportunities of ResearchingmelkyAinda não há avaliações
- Role of Quick Response To Supply ChainDocumento15 páginasRole of Quick Response To Supply ChainSanuwar RashidAinda não há avaliações
- Sample Database of SQL in Mysql FormatDocumento7 páginasSample Database of SQL in Mysql FormatsakonokeAinda não há avaliações
- Making Sense of The Future of Libraries: Dan Dorner, Jennifer Campbell-Meier and Iva SetoDocumento14 páginasMaking Sense of The Future of Libraries: Dan Dorner, Jennifer Campbell-Meier and Iva SetoBiblioteca IICEAinda não há avaliações
- Steinecker Boreas: Wort Stripping of The New GenerationDocumento16 páginasSteinecker Boreas: Wort Stripping of The New GenerationAlejandro Javier Delgado AraujoAinda não há avaliações
- Where Business Happens Where Happens: SupportDocumento19 páginasWhere Business Happens Where Happens: SupportRahul RamtekkarAinda não há avaliações
- FWN Magazine 2018 - Leonor VintervollDocumento48 páginasFWN Magazine 2018 - Leonor VintervollFilipina Women's NetworkAinda não há avaliações
- List of Every National School Walkout PDF LinksDocumento373 páginasList of Every National School Walkout PDF LinksStephanie Dube Dwilson100% (1)
- Zoomlion Gulf FZE Introduction: 1.1 ME Service Support 1.2 Construction CasesDocumento13 páginasZoomlion Gulf FZE Introduction: 1.1 ME Service Support 1.2 Construction CasesArk TradingAinda não há avaliações
- Skin Care Creams, Lotions and Gels For Cosmetic Use - SpecificationDocumento33 páginasSkin Care Creams, Lotions and Gels For Cosmetic Use - SpecificationJona Phie Montero NdtcnursingAinda não há avaliações
- Digital-To-Analog Converter - Wikipedia, The Free EncyclopediaDocumento8 páginasDigital-To-Analog Converter - Wikipedia, The Free EncyclopediaAnilkumar KubasadAinda não há avaliações
- Caracterisation D'une Entreprise anglosaxonne-ETLV - STMG1.Documento2 páginasCaracterisation D'une Entreprise anglosaxonne-ETLV - STMG1.meredith.licagaAinda não há avaliações
- Val Ed SyllabusDocumento25 páginasVal Ed Syllabusroy piamonteAinda não há avaliações
- LS3954A LS3954 LS3955 LS3956 LS3958: Linear Integrated SystemsDocumento3 páginasLS3954A LS3954 LS3955 LS3956 LS3958: Linear Integrated SystemsJCMAinda não há avaliações
- Omegas Prezentacija 01Documento20 páginasOmegas Prezentacija 01Predrag Djordjevic100% (1)
- Poster@IcepeDocumento1 páginaPoster@IcepeAakash NawabAinda não há avaliações
- 033 - Flight Planning Monitoring - QuestionsDocumento126 páginas033 - Flight Planning Monitoring - QuestionsEASA ATPL Question Bank100% (4)
- Plant Gardening AerationDocumento4 páginasPlant Gardening Aerationut.testbox7243Ainda não há avaliações
- GRADE 1 MUSIC Week 1 Learning PacketsDocumento16 páginasGRADE 1 MUSIC Week 1 Learning PacketsQuennie Rose EderAinda não há avaliações
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)