Você também pode gostar
- Specifications of S8 - ComenDocumento7 páginasSpecifications of S8 - ComenJuan Esteban F.100% (1)
- Placenta Previa NCP 1Documento6 páginasPlacenta Previa NCP 1Madhu Bala100% (1)
- Myocardial Infarction (MI)Documento23 páginasMyocardial Infarction (MI)Abedin Mehmedovic88% (60)
- NCP Cva Ineffective Tissue PerfusionDocumento1 páginaNCP Cva Ineffective Tissue Perfusionexcel21121Ainda não há avaliações
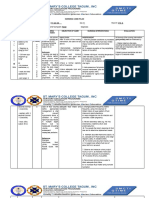
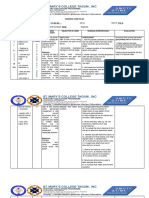
- Date/Tim e Cues Needs Nursing Diagnosis Scientific Basis Goals Objectives Criteria Nursing Interventions Rationale EvaluationDocumento7 páginasDate/Tim e Cues Needs Nursing Diagnosis Scientific Basis Goals Objectives Criteria Nursing Interventions Rationale EvaluationpjcolitaAinda não há avaliações
- Nursing Diagnosis Analysis Goal & Objectives Nursing Intervention Rationale EvaluationDocumento2 páginasNursing Diagnosis Analysis Goal & Objectives Nursing Intervention Rationale EvaluationLP BenozaAinda não há avaliações
- Assesncp DehydrationDocumento4 páginasAssesncp DehydrationVal FielAinda não há avaliações
- NCP For HypoDocumento5 páginasNCP For HypoCecil MonteroAinda não há avaliações
- NCP Sit. 2Documento3 páginasNCP Sit. 2Jay Debby RuizoAinda não há avaliações
- NCP - Tissue PerfusionDocumento3 páginasNCP - Tissue PerfusionFretzgine Lou ManuelAinda não há avaliações
- Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationDocumento3 páginasAssessment Nursing Diagnosis Planning Implementation Rationale EvaluationChloie Marie RosalejosAinda não há avaliações
- Case Study NCP ActualDocumento3 páginasCase Study NCP Actualdhamy florAinda não há avaliações
- NCP Impaired Cerebral Tissue PerfussionDocumento4 páginasNCP Impaired Cerebral Tissue PerfussionYvonne Ronamae100% (2)
- NCP&SOAPIEDocumento4 páginasNCP&SOAPIEMica OmotsosircAinda não há avaliações
- Diabetes Mellitus (DM)Documento1 páginaDiabetes Mellitus (DM)Bheru LalAinda não há avaliações
- NCP For DENGUEDocumento2 páginasNCP For DENGUEReina FernandezAinda não há avaliações
- Hyperthermia NCPDocumento3 páginasHyperthermia NCPkaylejordan_29100% (2)
- 1 NCP and 2 Drug StudyDocumento3 páginas1 NCP and 2 Drug StudyCristyl Shine BariaoAinda não há avaliações
- ROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPDocumento6 páginasROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPkimberly quitonAinda não há avaliações
- Short NoteDocumento43 páginasShort NotemulugetaAinda não há avaliações
- Nursing Care PlanDocumento13 páginasNursing Care PlanRen DolosaAinda não há avaliações
- NCP Ineffective Tissue PerfusionDocumento1 páginaNCP Ineffective Tissue PerfusionLEONELLGABRIEL RAGUINDINAinda não há avaliações
- Ectopic Pregnancy Nursing Care PlansDocumento27 páginasEctopic Pregnancy Nursing Care Plansviper7967880% (20)
- Nursing Care Plan Risk For Imbalance Body TemperatureDocumento4 páginasNursing Care Plan Risk For Imbalance Body TemperatureCarl J.Ainda não há avaliações
- Hyperthermia NCPDocumento2 páginasHyperthermia NCPmahangin85% (20)
- Lahore School of Nursing The University of Lahore Nursing Care PlanDocumento2 páginasLahore School of Nursing The University of Lahore Nursing Care PlanAyesha ImtiazAinda não há avaliações
- Cues Nursing Diagnosis Analysis Goal Nursing Intervention Rationale EvaluationDocumento5 páginasCues Nursing Diagnosis Analysis Goal Nursing Intervention Rationale Evaluationccchelle14Ainda não há avaliações
- Renal Failure NCPDocumento3 páginasRenal Failure NCPJet Ray-Ann GaringanAinda não há avaliações
- NCP KateDor NewDocumento6 páginasNCP KateDor NewSteffi GolezAinda não há avaliações
- NCP Case 3Documento3 páginasNCP Case 3boomer SeargeAinda não há avaliações
- Hyperthermia Drug StudyDocumento2 páginasHyperthermia Drug StudyTipey SegismundoAinda não há avaliações
- NCP IcuDocumento6 páginasNCP IcuLevyanne GsanchezAinda não há avaliações
- NCPDocumento6 páginasNCPLevyanne GsanchezAinda não há avaliações
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Subjective Short Term IndependentDocumento3 páginasAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Subjective Short Term IndependentMoi Valdoz100% (1)
- NCP and Drug Study (Isph-Gs Nursery)Documento4 páginasNCP and Drug Study (Isph-Gs Nursery)Cristyl Shine BariaoAinda não há avaliações
- Adrian G. Mallar BSN 2 Focus: Chest Pain Nursing Care Plan - Rheumatic Heart DiseaseDocumento3 páginasAdrian G. Mallar BSN 2 Focus: Chest Pain Nursing Care Plan - Rheumatic Heart DiseaseFarzana AfrinAinda não há avaliações
- Gi-Rle - NCP For Deficient Fluid VolumeDocumento2 páginasGi-Rle - NCP For Deficient Fluid VolumeEvangeline Villa de Gracia100% (1)
- SNU49Documento2 páginasSNU49Nora BacolAinda não há avaliações
- VILLAHERMOSA - Anorexia NCPDocumento9 páginasVILLAHERMOSA - Anorexia NCPJv Jore VillahermosaAinda não há avaliações
- Nursing Care PlanDocumento4 páginasNursing Care PlanNicolette BagasbasAinda não há avaliações
- NCP No. 2Documento2 páginasNCP No. 2Lorraine Tuesday BuenviajeAinda não há avaliações
- Nursing Care PlanDocumento4 páginasNursing Care PlanNicolette BagasbasAinda não há avaliações
- NCP Deficit Fluid VolumeDocumento4 páginasNCP Deficit Fluid VolumeKingJayson Pacman06Ainda não há avaliações
- HYPONATREMIADocumento3 páginasHYPONATREMIADienizs Labini TadenaAinda não há avaliações
- Ineffective Tissue Perfusion - NCPDocumento7 páginasIneffective Tissue Perfusion - NCPVianah Eve EscobidoAinda não há avaliações
- Dengue NCP PediaDocumento3 páginasDengue NCP Pediaraven riveraAinda não há avaliações
- Pedia Cases NCPDocumento27 páginasPedia Cases NCPDivine LavaAinda não há avaliações
- Assessment Cues Nursing Diagnosis Desired Outcome Nursing Intervention Justification EvaluationDocumento3 páginasAssessment Cues Nursing Diagnosis Desired Outcome Nursing Intervention Justification EvaluationKristil ChavezAinda não há avaliações
- PF EndocrineDocumento3 páginasPF EndocrinellocopoloAinda não há avaliações
- NCP Ineffective Tissue PerfusionDocumento4 páginasNCP Ineffective Tissue PerfusionSteffiAinda não há avaliações
- NCP Ineffective Tissue PerfusionDocumento4 páginasNCP Ineffective Tissue PerfusionSteffiAinda não há avaliações
- NCPDocumento7 páginasNCPTroy MirandaAinda não há avaliações
- Vital Signs Module 2Documento25 páginasVital Signs Module 2taekook is realAinda não há avaliações
- Ineffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesDocumento7 páginasIneffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesLouie ParillaAinda não há avaliações
- Cues Objectives Interventions Rationale Evaluation: Nursing Care PlanDocumento7 páginasCues Objectives Interventions Rationale Evaluation: Nursing Care PlanJulianne B. Dela CruzAinda não há avaliações
- 17Documento3 páginas17elvie21Ainda não há avaliações
- NCP TorresDocumento7 páginasNCP TorresbabiAinda não há avaliações
- Heart of the Field "Refresher & Nha Certification Quick Notes"No EverandHeart of the Field "Refresher & Nha Certification Quick Notes"Ainda não há avaliações
- O Level Biology Practice Questions And Answers HomeostasisNo EverandO Level Biology Practice Questions And Answers HomeostasisNota: 5 de 5 estrelas5/5 (1)
- GE Discovery VCT BrochureDocumento11 páginasGE Discovery VCT Brochurerabbani.moAinda não há avaliações
- ELSO Guideline Elso .1 PediatricDocumento5 páginasELSO Guideline Elso .1 Pediatricyowewe7363Ainda não há avaliações
- Duration of Dual Antiplatelet Therapy: Current ControversiesDocumento8 páginasDuration of Dual Antiplatelet Therapy: Current ControversiesRajendra ChavanAinda não há avaliações
- NURS FPX 6614 Assessment 1 Defining A Gap in PracticeDocumento6 páginasNURS FPX 6614 Assessment 1 Defining A Gap in Practicefarwaamjad771Ainda não há avaliações
- SonoAce - R7 - Reference Manual - EDocumento230 páginasSonoAce - R7 - Reference Manual - EEcomedical PlussAinda não há avaliações
- Cardiology Teaching PackageDocumento13 páginasCardiology Teaching Packagesarah morleyAinda não há avaliações
- Adobe Scan 13 May 2021Documento5 páginasAdobe Scan 13 May 2021Harisree SAinda não há avaliações
- Chapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartDocumento53 páginasChapter 4 - Normal and Anomalous Coronary Arteries in Humans. PartSaifuddin HaswareAinda não há avaliações
- الوحده الثالثهDocumento8 páginasالوحده الثالثهHUAWEI HUAWEI100% (1)
- Apical Four Chamber Echocardiogram ViewDocumento6 páginasApical Four Chamber Echocardiogram ViewMaria EdelAinda não há avaliações
- 2011 Acls Pretest Annotated Answer KeyDocumento20 páginas2011 Acls Pretest Annotated Answer Keyroro_maria_ulfahAinda não há avaliações
- Computation of Drips: Marla Aurora JacobaDocumento18 páginasComputation of Drips: Marla Aurora JacobaAnne Lorraine Bringas100% (1)
- Comparison of Dabigatran Versus Warfarin TreatmentDocumento7 páginasComparison of Dabigatran Versus Warfarin TreatmentDivyesh AmarsedaAinda não há avaliações
- 10 1161@hypertensionaha 119 14240 PDFDocumento8 páginas10 1161@hypertensionaha 119 14240 PDFAbidia KamilAinda não há avaliações
- New Recommendations According To 2022 ILCOR CoSTDocumento1 páginaNew Recommendations According To 2022 ILCOR CoSTMineTagraAinda não há avaliações
- Registration Form: Name of ChildDocumento5 páginasRegistration Form: Name of ChildỌsẹmwegie-Ẹro IrrediaAinda não há avaliações
- Adrenaline - EpinephrineDocumento3 páginasAdrenaline - Epinephrinesweety DangiAinda não há avaliações
- Heart Blocks: "The Heart Block Poem"Documento18 páginasHeart Blocks: "The Heart Block Poem"Bijay Kumar Mahato100% (1)
- ECG QuizDocumento6 páginasECG QuizIsland Rae100% (1)
- Cardiac Enzymes (Cardiac Biomarkers)Documento9 páginasCardiac Enzymes (Cardiac Biomarkers)Ahmad AfghanAinda não há avaliações
- Function and Importance of The Cardiovascular SystemDocumento3 páginasFunction and Importance of The Cardiovascular SystemBenjamin SmithAinda não há avaliações
- Comprehensive Case Study On Pulmonary Embolism: Prepared byDocumento17 páginasComprehensive Case Study On Pulmonary Embolism: Prepared byKristopher John JimenezAinda não há avaliações
- Structure and Function of The Cardiovascular System PDFDocumento9 páginasStructure and Function of The Cardiovascular System PDFteuuuuAinda não há avaliações
- Advanced Cardiac Life Support (ACLS)Documento17 páginasAdvanced Cardiac Life Support (ACLS)Siti Rahima HarahapAinda não há avaliações
- Vertebrobasilar Insufficiency/Syndrome: Hitesh Rohit (3 Year BPT)Documento14 páginasVertebrobasilar Insufficiency/Syndrome: Hitesh Rohit (3 Year BPT)Hitesh N RohitAinda não há avaliações
- Pathopharm Drug Tables Nclex ReviewDocumento65 páginasPathopharm Drug Tables Nclex ReviewRuiqi YangAinda não há avaliações
- Parameters of Fluid Responsiveness Curr Op Crit Care Shi2020Documento8 páginasParameters of Fluid Responsiveness Curr Op Crit Care Shi2020Tadeo PradoAinda não há avaliações
- Nursing Care Plan2Documento3 páginasNursing Care Plan2Fc CrisostomoAinda não há avaliações