Você também pode gostar
- ABEFIT - Stimulation ZoneDocumento9 páginasABEFIT - Stimulation ZonesoriboAinda não há avaliações
- Parts & Functions of Digestive SystemDocumento54 páginasParts & Functions of Digestive SystemRoyo Mel100% (1)
- GIT Physiology CHAPTER NO 62 Guyton by Dr. RoomiDocumento41 páginasGIT Physiology CHAPTER NO 62 Guyton by Dr. RoomiMudassar Roomi86% (14)
- ABO Incompatibility in NewbornsDocumento4 páginasABO Incompatibility in NewbornsNollen LaquianAinda não há avaliações
- Hemolytic Disease of NewbornDocumento14 páginasHemolytic Disease of NewbornAradhanaRamchandaniAinda não há avaliações
- Urinary Tract InfectionsDocumento6 páginasUrinary Tract Infectionspat_tienmin4552Ainda não há avaliações
- The Child With Hematologic DisordersDocumento149 páginasThe Child With Hematologic DisordersNics FranciscoAinda não há avaliações
- Respiratory System QuizDocumento8 páginasRespiratory System QuizJenny Dang100% (1)
- ABO Incompatibility in Newborns ExplainedDocumento9 páginasABO Incompatibility in Newborns ExplainedJuli-anne Villarico AndresAinda não há avaliações
- RH IncompatibilityDocumento7 páginasRH IncompatibilityMichael CabiliAinda não há avaliações
- DiarrheaDocumento38 páginasDiarrheaSTEPHANIE SOR100% (1)
- RH and Abo IncompatibilityDocumento10 páginasRH and Abo IncompatibilityamitAinda não há avaliações
- HELLP Concept Map RevisedDocumento1 páginaHELLP Concept Map RevisedwandaAinda não há avaliações
- Pregnancy Induced Hypertension Case StudyDocumento4 páginasPregnancy Induced Hypertension Case StudyMae Arra Lecobu-anAinda não há avaliações
- ICSE Class 10 Circulatory System NotesDocumento4 páginasICSE Class 10 Circulatory System NotesYash GuptaAinda não há avaliações
- Case Report Non-infection Unit Β-Major ThalassemiaDocumento27 páginasCase Report Non-infection Unit Β-Major ThalassemiaimamkdAinda não há avaliações
- Improve Memory with Yoga BreathingDocumento5 páginasImprove Memory with Yoga Breathingsugu61Ainda não há avaliações
- Abruptio PlacentaDocumento3 páginasAbruptio PlacentaNano KaAinda não há avaliações
- ABO BLOOD TYPE INCOMPATIBILITYDocumento58 páginasABO BLOOD TYPE INCOMPATIBILITYMichael John VallaritAinda não há avaliações
- Idiopathic Thrombocytopenic PurpuraDocumento8 páginasIdiopathic Thrombocytopenic PurpuraMonette Abalos MendovaAinda não há avaliações
- ABO Blood Group System ExplainedDocumento17 páginasABO Blood Group System ExplainedSYED MUHAMMAD ALI100% (1)
- Erythroblastosis FetalisDocumento10 páginasErythroblastosis Fetalissusan_grace123Ainda não há avaliações
- Hemolytic Disease of The Newborn: (Erythroblastosis Fetalis)Documento17 páginasHemolytic Disease of The Newborn: (Erythroblastosis Fetalis)sandeepv08Ainda não há avaliações
- Abo IncompatabilityDocumento3 páginasAbo Incompatabilityx483xDAinda não há avaliações
- Maternal antibodies attack fetal red blood cells in HDNDocumento7 páginasMaternal antibodies attack fetal red blood cells in HDNLara CarisaAinda não há avaliações
- RH Disease and ABO IncompatibilityDocumento21 páginasRH Disease and ABO Incompatibilityjeezislove617Ainda não há avaliações
- Causes and Symptoms of Beta-ThalassemiaDocumento1 páginaCauses and Symptoms of Beta-ThalassemiaAngie LamoAinda não há avaliações
- Ectopic PregDocumento6 páginasEctopic PregYwagar Ywagar0% (1)
- Pulmonary Atresia With Ventricular Septal Defect: Systematic ReviewDocumento10 páginasPulmonary Atresia With Ventricular Septal Defect: Systematic ReviewIvan VeriswanAinda não há avaliações
- Hemolytic Disease of NewbornDocumento15 páginasHemolytic Disease of Newborncyphochilus100% (1)
- Thalassemia Case StudyDocumento13 páginasThalassemia Case StudyNellyWataAinda não há avaliações
- Hemolytic AnemiaDocumento61 páginasHemolytic AnemiaMangayarkarasi ChandrakasanAinda não há avaliações
- FBCDocumento14 páginasFBCJane GarciaAinda não há avaliações
- Newborn Screening Policy Catarman Doctors Hospital, Inc.: University of Eastern PhilippinesDocumento7 páginasNewborn Screening Policy Catarman Doctors Hospital, Inc.: University of Eastern PhilippinesGenn Medrano GirayAinda não há avaliações
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocumento4 páginasIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezAinda não há avaliações
- Minggu 5 LP THALASSEMIADocumento14 páginasMinggu 5 LP THALASSEMIAMuhammad PanduAinda não há avaliações
- Mechanism of HypertensionDocumento4 páginasMechanism of HypertensionAlya Putri KhairaniAinda não há avaliações
- RevalidaDocumento5 páginasRevalidaHawkins FletcherAinda não há avaliações
- Hanta Vi Ru S Inf Ection SDocumento20 páginasHanta Vi Ru S Inf Ection Stummalapalli venkateswara rao100% (3)
- Hemolytic DiseaseDocumento10 páginasHemolytic DiseaseChino Paolo SamsonAinda não há avaliações
- MeaslesDocumento32 páginasMeaslesYum C100% (2)
- Dystocia: A Case PresentationDocumento63 páginasDystocia: A Case PresentationRoxanneGailBigcasGoleroAinda não há avaliações
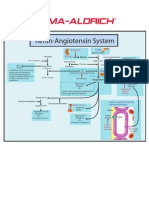
- Renin-Angiotensin SystemDocumento1 páginaRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Digestive System Guide: Parts & Functions Explained in 40 CharactersDocumento3 páginasDigestive System Guide: Parts & Functions Explained in 40 CharactersAziah Gan ManAinda não há avaliações
- Neonatal Jaundice Case Study: Early Diagnosis and Treatment Prevents Brain DamageDocumento6 páginasNeonatal Jaundice Case Study: Early Diagnosis and Treatment Prevents Brain DamagemuzamirAinda não há avaliações
- Pharma - Drugs Affecting Git MotilityDocumento6 páginasPharma - Drugs Affecting Git MotilityBobet ReñaAinda não há avaliações
- Surgery Case AppendicitisDocumento30 páginasSurgery Case AppendicitisSarahAinda não há avaliações
- Hydatidiform MoleDocumento10 páginasHydatidiform MoleLisa TurnerAinda não há avaliações
- Pku AlkDocumento33 páginasPku AlkSharf WangAinda não há avaliações
- (MID) IMMUNOSERO - Chapter 13 - Hypersensitivity (Reviewer)Documento6 páginas(MID) IMMUNOSERO - Chapter 13 - Hypersensitivity (Reviewer)Aisle Malibiran PalerAinda não há avaliações
- Food-Related Illnesses and Allergies (New)Documento57 páginasFood-Related Illnesses and Allergies (New)coosa liquorsAinda não há avaliações
- PKD Pathophysiology: How Polycystic Kidney Disease Causes Renal and Extrarenal ComplicationsDocumento2 páginasPKD Pathophysiology: How Polycystic Kidney Disease Causes Renal and Extrarenal Complicationsacey torreAinda não há avaliações
- SchistosomiasisDocumento33 páginasSchistosomiasishendra ari100% (1)
- Stem Cells EssayDocumento4 páginasStem Cells EssayalskjdhhAinda não há avaliações
- Acute Glomerulonephritis Case StudyDocumento6 páginasAcute Glomerulonephritis Case StudyjakerzAinda não há avaliações
- Type B (Hib) Vaccine: Haemophilus InfluenzaeDocumento2 páginasType B (Hib) Vaccine: Haemophilus InfluenzaeEnce MalatambanAinda não há avaliações
- Amniotic Fluid EmbolismDocumento16 páginasAmniotic Fluid EmbolismAbdul Hamid Alraiyes100% (4)
- Are Viruses Living or Non-Living Organisms?Documento8 páginasAre Viruses Living or Non-Living Organisms?Sydney Cloyce NagalAinda não há avaliações
- Dilute Russell's Viper Venom Test (dRVVT) ExplainedDocumento15 páginasDilute Russell's Viper Venom Test (dRVVT) ExplainedAngelo GreenAinda não há avaliações
- Biochemistry of GlycoproteinDocumento6 páginasBiochemistry of GlycoproteinMahathir Mohmed100% (7)
- Fluid Volume Deficit and Excess: Types, Causes, Signs and Nursing ManagementDocumento32 páginasFluid Volume Deficit and Excess: Types, Causes, Signs and Nursing ManagementAcohCChaoAinda não há avaliações
- Medical Laboratory Technology: I. Short Notes, Answer Any FOUR Questions. 4 X 5 20 MarksDocumento60 páginasMedical Laboratory Technology: I. Short Notes, Answer Any FOUR Questions. 4 X 5 20 MarksSrikutty DevuAinda não há avaliações
- Antiphospholipid Syndrome (Aps) and PregnancyDocumento36 páginasAntiphospholipid Syndrome (Aps) and Pregnancyskeisham11Ainda não há avaliações
- Problem-based Approach to Gastroenterology and HepatologyNo EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisAinda não há avaliações
- Erythroblastosis FetalisDocumento4 páginasErythroblastosis FetalisGeorgina ErfeAinda não há avaliações
- Hemolytic Diseases of The Fetus and NewbornDocumento30 páginasHemolytic Diseases of The Fetus and Newbornkristine_camerinoAinda não há avaliações
- Human Body Review TestDocumento6 páginasHuman Body Review TestMrCiambroneAinda não há avaliações
- Percussion:: o o o o oDocumento2 páginasPercussion:: o o o o oAnonymous b4P7PDAinda não há avaliações
- Hemolytic Anemia IIDocumento18 páginasHemolytic Anemia IIrizuka-chanAinda não há avaliações
- Struktur Hewan Anatomi 1Documento6 páginasStruktur Hewan Anatomi 1Devina AlifahAinda não há avaliações
- Life Process AssignmentDocumento3 páginasLife Process AssignmentJyoti SethiAinda não há avaliações
- Strengthening and Benefits of Bridge PoseDocumento5 páginasStrengthening and Benefits of Bridge PosekovelrAinda não há avaliações
- Quiz 1: Key Life Processes And Human Body Organization (40chDocumento11 páginasQuiz 1: Key Life Processes And Human Body Organization (40chJackson JastariAinda não há avaliações
- The Respiratory System: Part ADocumento58 páginasThe Respiratory System: Part ASophia LawrenceAinda não há avaliações
- Cu 10 (Ncma111)Documento2 páginasCu 10 (Ncma111)Arjay VerdejoAinda não há avaliações
- Lesson Plan No. 3Documento6 páginasLesson Plan No. 3Pineda RenzAinda não há avaliações
- Respiratory Assessment LandmarksDocumento15 páginasRespiratory Assessment LandmarksChilled Moo MooAinda não há avaliações
- Unit 7 AP Biology Study GuideDocumento3 páginasUnit 7 AP Biology Study GuideTootsieAinda não há avaliações
- Vital Signs Monitoring GuideDocumento107 páginasVital Signs Monitoring GuidesubiAinda não há avaliações
- MS LAB Oxygenation Nursing SkillsDocumento9 páginasMS LAB Oxygenation Nursing SkillsRouwi DesiatcoAinda não há avaliações
- Self-Learning Module For Grade 11: Earth and Life Science How Animals Survive How Will You Use This Module?Documento8 páginasSelf-Learning Module For Grade 11: Earth and Life Science How Animals Survive How Will You Use This Module?MIMOYOUAinda não há avaliações
- Understanding Obstructive Sleep Apnea: Causes, Symptoms, and Treatment OptionsDocumento27 páginasUnderstanding Obstructive Sleep Apnea: Causes, Symptoms, and Treatment OptionsdammieboiAinda não há avaliações
- Blood 2Documento13 páginasBlood 2abbaslafeAinda não há avaliações
- Practical Journals I II III IV BAMS 120115Documento229 páginasPractical Journals I II III IV BAMS 120115aarogyaAinda não há avaliações
- Lesson Plan in ScienceDocumento3 páginasLesson Plan in SciencePRINCESS ANGELLA SITUBALAinda não há avaliações
- Fha Respirasi Bu Fani b03Documento35 páginasFha Respirasi Bu Fani b03shofurawijayantiAinda não há avaliações
- Schools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasDocumento2 páginasSchools Division of Negros Oriental: Republic of The Philippines Region VII, Central VisayasSharna Flynn SolonAinda não há avaliações
- Self Assessment LifestyleDocumento4 páginasSelf Assessment LifestyleBettyAinda não há avaliações
- Death and Dying/terminology: Hospice Postmortem Care Rigor Mortis Death Rattle MoribundDocumento45 páginasDeath and Dying/terminology: Hospice Postmortem Care Rigor Mortis Death Rattle MoribundFinisiska Dwi Asti RAinda não há avaliações
- Blood functions and testingDocumento4 páginasBlood functions and testingred8blue8Ainda não há avaliações