Você também pode gostar
- 2023 OB/GYN Coding Manual: Components of Correct CodingNo Everand2023 OB/GYN Coding Manual: Components of Correct CodingAinda não há avaliações
- 2Documento11 páginas2smilingeyes_nicAinda não há avaliações
- Roils PaperDocumento4 páginasRoils Paperapi-569210408Ainda não há avaliações
- The Impact of COVID 19 On Patient Preferences in An Orthopaedic ClinicDocumento10 páginasThe Impact of COVID 19 On Patient Preferences in An Orthopaedic ClinicAthenaeum Scientific PublishersAinda não há avaliações
- Research On Medical EthicsDocumento4 páginasResearch On Medical EthicsRatneshAinda não há avaliações
- Ethics IndiaDocumento4 páginasEthics IndialamyaaAinda não há avaliações
- 80 RecommendationDocumento16 páginas80 Recommendationarthik603Ainda não há avaliações
- 89 312 2 PB PDFDocumento8 páginas89 312 2 PB PDFAnonymous gw6mqMC7KAinda não há avaliações
- CroaciaDocumento5 páginasCroaciaMariano SalvadorAinda não há avaliações
- 408 1157 1 PBDocumento9 páginas408 1157 1 PBUPTPKM WringinanomAinda não há avaliações
- AJMSOA-23-91123@Q2 ApprovedDocumento11 páginasAJMSOA-23-91123@Q2 ApprovedTibebu TilahunAinda não há avaliações
- H Chandwani, P Jivarajani, H JivarajaniDocumento8 páginasH Chandwani, P Jivarajani, H JivarajaniakmohideenAinda não há avaliações
- Analisa Deskriptif Pelaksanaan Dan Kelengkapan Informed Consent Tindakan Ect Premedikasi Pada DRM Pasien Gangguan JiwaDocumento12 páginasAnalisa Deskriptif Pelaksanaan Dan Kelengkapan Informed Consent Tindakan Ect Premedikasi Pada DRM Pasien Gangguan JiwaNova Dwi Pawestri IIAinda não há avaliações
- Knowledge, Awareness, and Attitude Toward DentalDocumento4 páginasKnowledge, Awareness, and Attitude Toward DentalMax FaxAinda não há avaliações
- The Problem and Review of Related Literature and StudiesDocumento36 páginasThe Problem and Review of Related Literature and StudiesCJ AngelesAinda não há avaliações
- RoilsDocumento4 páginasRoilsapi-568855135Ainda não há avaliações
- JournalDocumento8 páginasJournalCanam, Allysa F.Ainda não há avaliações
- Knowlegde and Willingness To Donate Eye Among Medical Doctors in Delta StateDocumento7 páginasKnowlegde and Willingness To Donate Eye Among Medical Doctors in Delta StateInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Abbo 2011Documento6 páginasAbbo 2011Mohibbul HaqueAinda não há avaliações
- Drug Prescribing Pattern in Surgical Wards of A TeDocumento6 páginasDrug Prescribing Pattern in Surgical Wards of A TeNiranjan ChapagainAinda não há avaliações
- Torts CIA 1Documento5 páginasTorts CIA 1Amayra DixitAinda não há avaliações
- Dentist-Patient Communication As Perceived by Patients in Riyadh, Saudi ArabiaDocumento8 páginasDentist-Patient Communication As Perceived by Patients in Riyadh, Saudi ArabiaNisa HassanAinda não há avaliações
- Surgeons Want Improvements, Survey SaysDocumento2 páginasSurgeons Want Improvements, Survey SaysisidromcAinda não há avaliações
- HSJ Vol.6no.2 2017-45-49Documento5 páginasHSJ Vol.6no.2 2017-45-49Mario CabreraAinda não há avaliações
- Patients Rights and ResponsibilitiesDocumento18 páginasPatients Rights and ResponsibilitiesmuthurajathiAinda não há avaliações
- Informed Consent For Elective and Emergency Surgery: Questionnaire StudyDocumento6 páginasInformed Consent For Elective and Emergency Surgery: Questionnaire StudyNoviAinda não há avaliações
- 2018 Consumer Study Updated 002Documento24 páginas2018 Consumer Study Updated 002Alaa AhmedAinda não há avaliações
- 1 PDFDocumento19 páginas1 PDFDoni DarcoAinda não há avaliações
- Doctor Shopping Behaviour and Its Predisposing Factors Amongst Dermatology PatientsDocumento6 páginasDoctor Shopping Behaviour and Its Predisposing Factors Amongst Dermatology PatientsNugi AshterAinda não há avaliações
- Patient Satisfaction With Telehealth Vs Inperson Hand Therapy A Retrospective Review of Results of An Online Satisfaction SurveyDocumento7 páginasPatient Satisfaction With Telehealth Vs Inperson Hand Therapy A Retrospective Review of Results of An Online Satisfaction Surveyanita awAinda não há avaliações
- Adherence To Informed Consent Standards in Shiraz Hospitals: Matrons' PerspectiveDocumento6 páginasAdherence To Informed Consent Standards in Shiraz Hospitals: Matrons' PerspectiveLaxmi Kant SahaniAinda não há avaliações
- Quality of Informed Consent For Invasive ProceduresDocumento6 páginasQuality of Informed Consent For Invasive ProceduresMariana Conti OliveiraAinda não há avaliações
- Code of Professional Conduct (DR GG)Documento30 páginasCode of Professional Conduct (DR GG)Athirah AmranAinda não há avaliações
- Electronic Med Rec AOMDocumento25 páginasElectronic Med Rec AOMfatiisaadatAinda não há avaliações
- JournalDocumento6 páginasJournalkhaiz_142989Ainda não há avaliações
- Dapus 11Documento4 páginasDapus 11nadya salsabilaAinda não há avaliações
- Heri,+94 +Devi+Ristian+Octavia+713+783-792Documento10 páginasHeri,+94 +Devi+Ristian+Octavia+713+783-792Retno WahyuningrumAinda não há avaliações
- Continence AuditDocumento6 páginasContinence Auditi can always make u smile :DAinda não há avaliações
- Knowledge of Medical Certificate of CausDocumento7 páginasKnowledge of Medical Certificate of Causimrana.morshedAinda não há avaliações
- Towards Patient-Centered Care For People Living With Kidney DiseaseDocumento8 páginasTowards Patient-Centered Care For People Living With Kidney DiseaseEva RetniAinda não há avaliações
- Self Medication Among Patients Seen at Ophthalmology Clinics at Four Hospitals in Dar Es Salaam TanzaniaDocumento5 páginasSelf Medication Among Patients Seen at Ophthalmology Clinics at Four Hospitals in Dar Es Salaam TanzaniaIOSR Journal of PharmacyAinda não há avaliações
- Consent Adalah Persetujuan Yang Diberikan Pasien Atau Keluarga Atas DasarDocumento7 páginasConsent Adalah Persetujuan Yang Diberikan Pasien Atau Keluarga Atas DasarrezaAinda não há avaliações
- ADA Guidelines Consent For CareDocumento15 páginasADA Guidelines Consent For CareNikitha KanithiAinda não há avaliações
- Knowledge, Attitude, and Practices About Biomedical Waste Management Among Healthcare Personnel: A Cross-Sectional StudyDocumento5 páginasKnowledge, Attitude, and Practices About Biomedical Waste Management Among Healthcare Personnel: A Cross-Sectional StudyLa RikiAinda não há avaliações
- ADAPolicies 5-17 DentalRecordsDocumento10 páginasADAPolicies 5-17 DentalRecordshadia durani100% (1)
- Professional Med J Q 2013 20 6 973 980Documento8 páginasProfessional Med J Q 2013 20 6 973 980Vikram AripakaAinda não há avaliações
- Faculty of Nursing, Damietta University: Third YearDocumento8 páginasFaculty of Nursing, Damietta University: Third YearMagdy RamadanAinda não há avaliações
- RRL JordanDocumento6 páginasRRL JordanZllison Mae Teodoro MangabatAinda não há avaliações
- Knowledge and Practice Towards Prevention of Surgical Site Infection Among Healthcare Professionals in Buraidah City, Saudi ArabiaDocumento7 páginasKnowledge and Practice Towards Prevention of Surgical Site Infection Among Healthcare Professionals in Buraidah City, Saudi ArabiamajedAinda não há avaliações
- A Study On Out Patient Satisfaction at A Super Specialty Hospital in IndiaDocumento6 páginasA Study On Out Patient Satisfaction at A Super Specialty Hospital in IndiaVikram AripakaAinda não há avaliações
- Jurnal 1 Journal of PharmaceuticsDocumento15 páginasJurnal 1 Journal of Pharmaceuticsinter milanAinda não há avaliações
- Consent Tool KitDocumento46 páginasConsent Tool KitDexter SimAinda não há avaliações
- H+T QuizDocumento128 páginasH+T Quizrachel.m.johnson9780Ainda não há avaliações
- Management of Medical Records: Facts and Figures For SurgeonsDocumento4 páginasManagement of Medical Records: Facts and Figures For SurgeonsGerald SweinslionAinda não há avaliações
- Prevalence of Carpal Tunnel Syndrome Symptoms Among Dentists in Benghazi City - LibyaDocumento6 páginasPrevalence of Carpal Tunnel Syndrome Symptoms Among Dentists in Benghazi City - LibyaIJAR JOURNALAinda não há avaliações
- 2015 Patient-Satisfaction-From-Medical-Service-Provided-By-University-Outpatient-Clinic-Taif-University-Saudi-ArabiaDocumento8 páginas2015 Patient-Satisfaction-From-Medical-Service-Provided-By-University-Outpatient-Clinic-Taif-University-Saudi-Arabiaapouakone apouakoneAinda não há avaliações
- MainDocumento6 páginasMainBitter PanAinda não há avaliações
- Ambulatory Prescribing Errors Among Community Based Providers in Two StatesDocumento6 páginasAmbulatory Prescribing Errors Among Community Based Providers in Two StatesIsaura RubioAinda não há avaliações
- 145 324 1 SMDocumento6 páginas145 324 1 SMdiannoey74Ainda não há avaliações
- California Department of Housing and Community Development vs. City of Huntington BeachDocumento11 páginasCalifornia Department of Housing and Community Development vs. City of Huntington BeachThe Press-Enterprise / pressenterprise.comAinda não há avaliações
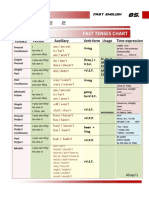
- Table 2: Fast Tenses ChartDocumento5 páginasTable 2: Fast Tenses ChartAngel Julian HernandezAinda não há avaliações
- Sikfil ReviewerDocumento6 páginasSikfil ReviewerBarrientos Lhea ShaineAinda não há avaliações
- A#2 8612 SehrishDocumento16 páginasA#2 8612 SehrishMehvish raniAinda não há avaliações
- 2nd Prelim ExamDocumento6 páginas2nd Prelim Exammechille lagoAinda não há avaliações
- Final Advert For The Blue Economy PostsDocumento5 páginasFinal Advert For The Blue Economy PostsKhan SefAinda não há avaliações
- Abnormal Psychology: A Case Study of Disco DiDocumento7 páginasAbnormal Psychology: A Case Study of Disco DiSarah AllahwalaAinda não há avaliações
- Military Laws in India - A Critical Analysis of The Enforcement Mechanism - IPleadersDocumento13 páginasMilitary Laws in India - A Critical Analysis of The Enforcement Mechanism - IPleadersEswar StarkAinda não há avaliações
- Test 6Documento7 páginasTest 6RuslanaAinda não há avaliações
- The Overseas Chinese of South East Asia: Ian Rae and Morgen WitzelDocumento178 páginasThe Overseas Chinese of South East Asia: Ian Rae and Morgen WitzelShukwai ChristineAinda não há avaliações
- (Mr. Nigel West, Oleg Tsarev) TRIPLEX Secrets Fro (B-Ok - Xyz)Documento377 páginas(Mr. Nigel West, Oleg Tsarev) TRIPLEX Secrets Fro (B-Ok - Xyz)conbeAinda não há avaliações
- 504 Loan Refinancing ProgramDocumento5 páginas504 Loan Refinancing ProgramPropertywizzAinda não há avaliações
- 09 Task Performance 1-ARG - ZABALA GROUPDocumento6 páginas09 Task Performance 1-ARG - ZABALA GROUPKylle Justin ZabalaAinda não há avaliações
- Final Report Class V - SLAS 15-16 PDFDocumento87 páginasFinal Report Class V - SLAS 15-16 PDFbhairav ghimireAinda não há avaliações
- Entrepreneurship: The Entrepreneur, The Individual That SteersDocumento11 páginasEntrepreneurship: The Entrepreneur, The Individual That SteersJohn Paulo Sayo0% (1)
- Farhat Ziadeh - Winds Blow Where Ships Do Not Wish To GoDocumento32 páginasFarhat Ziadeh - Winds Blow Where Ships Do Not Wish To GoabshlimonAinda não há avaliações
- Taking The Red Pill - The Real MatrixDocumento26 páginasTaking The Red Pill - The Real MatrixRod BullardAinda não há avaliações
- Discussion: Functions, Advantages and Disadvantages of BIOPOT Cassava Peel and Husk CharcoalDocumento4 páginasDiscussion: Functions, Advantages and Disadvantages of BIOPOT Cassava Peel and Husk CharcoalAhmad BurhanudinAinda não há avaliações
- Land Laws (MOHD AQIB SF)Documento18 páginasLand Laws (MOHD AQIB SF)Mohd AqibAinda não há avaliações
- Retail Strategy: MarketingDocumento14 páginasRetail Strategy: MarketingANVESHI SHARMAAinda não há avaliações
- 240 Marilag v. MartinezDocumento21 páginas240 Marilag v. Martinezdos2reqjAinda não há avaliações
- PDF Issue 1 PDFDocumento128 páginasPDF Issue 1 PDFfabrignani@yahoo.comAinda não há avaliações
- Timeline of American OccupationDocumento3 páginasTimeline of American OccupationHannibal F. Carado100% (3)
- Facilitators of Globalization PresentationDocumento3 páginasFacilitators of Globalization PresentationCleon Roxann WebbeAinda não há avaliações
- Questionnaire of Personal and Organizational Values Congruence For Employee (Q-POVC-115)Documento6 páginasQuestionnaire of Personal and Organizational Values Congruence For Employee (Q-POVC-115)Kowshik SAinda não há avaliações
- (East Central and Eastern Europe in the Middle Ages, 450-1450_ vol. 21) Paul Milliman-_The Slippery Memory of Men__ The Place of Pomerania in the Medieval Kingdom of Poland-Brill Academic Publishers (.pdfDocumento337 páginas(East Central and Eastern Europe in the Middle Ages, 450-1450_ vol. 21) Paul Milliman-_The Slippery Memory of Men__ The Place of Pomerania in the Medieval Kingdom of Poland-Brill Academic Publishers (.pdfRaphael BraunAinda não há avaliações
- BB 100 - Design For Fire Safety in SchoolsDocumento160 páginasBB 100 - Design For Fire Safety in SchoolsmyscriblkAinda não há avaliações
- Gouri MohammadDocumento3 páginasGouri MohammadMizana KabeerAinda não há avaliações
- ZodiacDocumento6 páginasZodiacapi-26172340Ainda não há avaliações
- Flipkart Labels 23 Apr 2024 10 18Documento4 páginasFlipkart Labels 23 Apr 2024 10 18Giri KanyakumariAinda não há avaliações