Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- LogDocumento7 páginasLogHerdi YantoAinda não há avaliações
- Rails BasicsDocumento229 páginasRails BasicsachhuAinda não há avaliações
- 1.17 - Surreptitious Software Obfuscation, Watermarking, and Tamperproofing For Software ProtectionDocumento1.041 páginas1.17 - Surreptitious Software Obfuscation, Watermarking, and Tamperproofing For Software ProtectionGabriel DiasAinda não há avaliações
- CAT Álogo de Peças de Reposi ÇÃO: Trator 5403Documento364 páginasCAT Álogo de Peças de Reposi ÇÃO: Trator 5403MARCOS DIONIS ALVES LIMAAinda não há avaliações
- DCS800 Firmware Manual EnglishDocumento298 páginasDCS800 Firmware Manual EnglishMadson FernandesAinda não há avaliações
- Compre Queation PaperDocumento6 páginasCompre Queation PaperGanesh DharmireddyAinda não há avaliações
- Operating and Maintenance Manual 322375H01 Rev CDocumento82 páginasOperating and Maintenance Manual 322375H01 Rev CGustavo BarbosaAinda não há avaliações
- 4july BookDocumento5 páginas4july BookDevansh AggarwalAinda não há avaliações
- Grammar 111Documento33 páginasGrammar 111Suntithvibol Sem100% (1)
- Digital Control SystemDocumento34 páginasDigital Control SystemLaxman Koirala100% (3)
- 13 EGWDC 2012 CompresscoDocumento17 páginas13 EGWDC 2012 CompresscoVeky Pamintu100% (1)
- Ethernet Managed Phoenix Contact 2702331 enDocumento25 páginasEthernet Managed Phoenix Contact 2702331 enshankar kumarAinda não há avaliações
- Postmodernity in PiDocumento2 páginasPostmodernity in Pixhardy27Ainda não há avaliações
- Minihydro GANZ enDocumento5 páginasMinihydro GANZ enRade NovakovicAinda não há avaliações
- Water Level Sensor (Submersible)Documento4 páginasWater Level Sensor (Submersible)anon_975837510Ainda não há avaliações
- Cortec, VpCI-371 Application GuideDocumento2 páginasCortec, VpCI-371 Application Guidemonserrat PereaAinda não há avaliações
- Module 3Documento10 páginasModule 3Michael godsonAinda não há avaliações
- ITTC Surface TreatmentDocumento63 páginasITTC Surface Treatments_brizzolaraAinda não há avaliações
- Introduction To Research MethodsDocumento11 páginasIntroduction To Research MethodsKamlakar SadavarteAinda não há avaliações
- Alarm ListDocumento4 páginasAlarm ListMirela Perenda ŠabićAinda não há avaliações
- Access Workshop 01Documento8 páginasAccess Workshop 01movogonAinda não há avaliações
- PDF Sesion de Aprendizaje de Comunicacion Leemos y Cantamos Canciones Criollas Lambayecanas - CompressDocumento6 páginasPDF Sesion de Aprendizaje de Comunicacion Leemos y Cantamos Canciones Criollas Lambayecanas - CompressJulia Navarro CheroAinda não há avaliações
- Temporal BroadeningDocumento10 páginasTemporal BroadeningMohamed BouhaddaAinda não há avaliações
- Basic Electronics (ES-112)Documento49 páginasBasic Electronics (ES-112)Bharat LalAinda não há avaliações
- 9 0 Development and OperatingDocumento12 páginas9 0 Development and OperatingAnu Partha100% (1)
- Pediatric Appendicitis ScoreDocumento6 páginasPediatric Appendicitis ScorePinandhito LatukolanAinda não há avaliações
- Mothballing Requires More Than Idle ThoughtDocumento4 páginasMothballing Requires More Than Idle Thoughtfawmer61Ainda não há avaliações
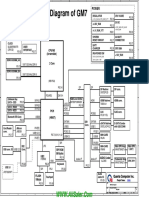
- Dell XPS 17 Quanta GM7 Rev D SchematicsDocumento39 páginasDell XPS 17 Quanta GM7 Rev D SchematicsvcompumatikAinda não há avaliações
- V-Ray For SketchUp Rendering An Exterior Scene PDFDocumento7 páginasV-Ray For SketchUp Rendering An Exterior Scene PDFDevohAinda não há avaliações
- MCAT Uhs Past Paper (2008-2016)Documento180 páginasMCAT Uhs Past Paper (2008-2016)Abdullah SheikhAinda não há avaliações