Você também pode gostar
- Laws and Patents in IndiaDocumento8 páginasLaws and Patents in IndiaMarudavanan SomasundaramAinda não há avaliações
- BOLAR EXEMPTION Under Indian Patent LawDocumento8 páginasBOLAR EXEMPTION Under Indian Patent LawTouch me NotAinda não há avaliações
- Patent Law ProjectDocumento6 páginasPatent Law ProjectJoachim SaldanhaAinda não há avaliações
- IP and Technology: Department of Biotechnology, IIT GuwahatiDocumento27 páginasIP and Technology: Department of Biotechnology, IIT GuwahatiAgradaAinda não há avaliações
- Presentation On Patents Act-1970 NewDocumento25 páginasPresentation On Patents Act-1970 NewNilesh ParekhAinda não há avaliações
- Chanakya National Law University: SUBMITTED TO: Ms. Nandita JhaDocumento13 páginasChanakya National Law University: SUBMITTED TO: Ms. Nandita JhaGauravPrakashAinda não há avaliações
- Presentation Compulsory Licensing 1Documento28 páginasPresentation Compulsory Licensing 1Rahul ChawlaAinda não há avaliações
- Patent Act 1970Documento16 páginasPatent Act 1970Shivam Bhasin0% (1)
- Final Ipr&Lp Book 10022020Documento480 páginasFinal Ipr&Lp Book 10022020UabajAinda não há avaliações
- Exclusion of Oral by DocumentaryDocumento21 páginasExclusion of Oral by Documentarysachet12Ainda não há avaliações
- MAnual of Patent in IndiaDocumento163 páginasMAnual of Patent in Indiaapi-37028980% (1)
- Anticipation & Secrecy DirectionsDocumento12 páginasAnticipation & Secrecy DirectionsBindu SharmaAinda não há avaliações
- Xavier University Xavier Law SchoolDocumento16 páginasXavier University Xavier Law Schoolsarayu alluAinda não há avaliações
- The Sui Generis Protection of The Plant Varieties Farmers Vs Breeders Rights in India SynopsisDocumento2 páginasThe Sui Generis Protection of The Plant Varieties Farmers Vs Breeders Rights in India SynopsisLegendAinda não há avaliações
- Chapter 2 - Patent - Background and Basic PrinciplesDocumento40 páginasChapter 2 - Patent - Background and Basic PrinciplesAshutosh Singh ParmarAinda não há avaliações
- Sociology ProjectDocumento21 páginasSociology ProjectRitika KukrejaAinda não há avaliações
- Vivek Kumar Sai Transferof Property - Sem IV.Documento18 páginasVivek Kumar Sai Transferof Property - Sem IV.Vivek SaiAinda não há avaliações
- Import Substitution and Export Promotion As Development StrategiesDocumento11 páginasImport Substitution and Export Promotion As Development StrategiesSuraj KumarAinda não há avaliações
- Assignment of Trademarks in IndiaDocumento4 páginasAssignment of Trademarks in IndiaKunal SharmaAinda não há avaliações
- Patent PDFDocumento63 páginasPatent PDFmonuAinda não há avaliações
- Product V Patent (2011)Documento21 páginasProduct V Patent (2011)jns198Ainda não há avaliações
- Aryan Kaushal - 15 Patent Law AssignmentDocumento19 páginasAryan Kaushal - 15 Patent Law AssignmentNilotpal RaiAinda não há avaliações
- IPR Regime in India Government InitiativesDocumento20 páginasIPR Regime in India Government InitiativesDipanshu KambojAinda não há avaliações
- History of Indian Patent SystemDocumento3 páginasHistory of Indian Patent SystemProf_WasimAinda não há avaliações
- IPR AssignmentDocumento13 páginasIPR AssignmentMeharobAinda não há avaliações
- Bhiwant Prasad Radhey ShyamDocumento15 páginasBhiwant Prasad Radhey ShyamAashish KohliAinda não há avaliações
- Possible Effect of TRIPS On Patent in IndiaDocumento10 páginasPossible Effect of TRIPS On Patent in IndiaLAW MANTRAAinda não há avaliações
- Section 3 (D) Indian Patent ActDocumento4 páginasSection 3 (D) Indian Patent ActRonak ParmarAinda não há avaliações
- WHAT IS PATENT?: Patent Is A Monopoly Granted by Statute of A Country For A Limited Term OverDocumento15 páginasWHAT IS PATENT?: Patent Is A Monopoly Granted by Statute of A Country For A Limited Term OverRajkumarKariAinda não há avaliações
- Intellectual Property RightsDocumento22 páginasIntellectual Property RightsSargam MohlaAinda não há avaliações
- Section 10 (4) of The Patents Act, 1970Documento6 páginasSection 10 (4) of The Patents Act, 1970sudhir.kochhar3530Ainda não há avaliações
- Dr. Ram Manohar Lohiya National Law University: Academic Year - 2020Documento12 páginasDr. Ram Manohar Lohiya National Law University: Academic Year - 2020Yamini SinghAinda não há avaliações
- Animal Cruelty and Protection in IndiaDocumento3 páginasAnimal Cruelty and Protection in IndiaSamarth NayarAinda não há avaliações
- Legal Education FinalDocumento18 páginasLegal Education FinalkulwinderkaurAinda não há avaliações
- Ipr 5Documento23 páginasIpr 5JIJO RAJAinda não há avaliações
- Concept of Patents Law in IndiaDocumento14 páginasConcept of Patents Law in IndiaMríñålÀryäñAinda não há avaliações
- 2.patent FeaturesDocumento15 páginas2.patent FeaturesAgradaAinda não há avaliações
- Ms. Kuhu Tiwari: Hidayatullah National Law UniversityDocumento20 páginasMs. Kuhu Tiwari: Hidayatullah National Law UniversityNaveen SihareAinda não há avaliações
- Rights and Obligations of The PatenteeDocumento11 páginasRights and Obligations of The PatenteeHumanyu KabeerAinda não há avaliações
- Intellectual Property Rights (Ipr) : Dr. Hemant BabhulkarDocumento46 páginasIntellectual Property Rights (Ipr) : Dr. Hemant BabhulkarHemant BabhulkarAinda não há avaliações
- Indian Patent ActDocumento51 páginasIndian Patent ActKuenzang Tshokyee SangeyAinda não há avaliações
- Intellectual Property LawsDocumento27 páginasIntellectual Property Lawsangel mathew100% (1)
- Economic Planning & Objectives & Reason Behind Failures of Economic PlanningDocumento3 páginasEconomic Planning & Objectives & Reason Behind Failures of Economic PlanningRashmi Ranjan Panigrahi100% (1)
- Chanakya National Law University, Patna: Project of Public International LawDocumento22 páginasChanakya National Law University, Patna: Project of Public International LawAditya Singh100% (1)
- Agreement On TradeDocumento28 páginasAgreement On TradepraharshithaAinda não há avaliações
- Note On Compulsory LicensingDocumento34 páginasNote On Compulsory LicensingSaksham GargAinda não há avaliações
- Trademark ActDocumento21 páginasTrademark ActSajan KumarAinda não há avaliações
- The Doctrine of Equivalents in Patent InfringementDocumento3 páginasThe Doctrine of Equivalents in Patent InfringementArpit JainAinda não há avaliações
- IPRDocumento10 páginasIPRpaulAinda não há avaliações
- Volume 3 Issue 1: Mr. Zubair Ahmed Guest Faculty and Research Scholar, Department of Law, Assam University, SilcharDocumento10 páginasVolume 3 Issue 1: Mr. Zubair Ahmed Guest Faculty and Research Scholar, Department of Law, Assam University, Silcharsaiby khanAinda não há avaliações
- History of Patent LawDocumento14 páginasHistory of Patent LawNasif MustahidAinda não há avaliações
- Legal Education and ResearchDocumento279 páginasLegal Education and Researchsemarang100% (1)
- IPR Seventh SemesterDocumento8 páginasIPR Seventh SemesterGunjan SinghAinda não há avaliações
- PDF Compulsory Licence in Patent Intellectual Property RightsDocumento16 páginasPDF Compulsory Licence in Patent Intellectual Property RightskartikAinda não há avaliações
- Evidence Law Project 1Documento21 páginasEvidence Law Project 1Nidhi PillayAinda não há avaliações
- SSSSSS: Doha Declaration: Compulsory Licensing and Access To Drugs/MedicinesDocumento14 páginasSSSSSS: Doha Declaration: Compulsory Licensing and Access To Drugs/MedicinesAnjaliAinda não há avaliações
- Sachin Yadav - IPR - 70Documento10 páginasSachin Yadav - IPR - 70abhinandan royAinda não há avaliações
- TRIPs & PatentsDocumento8 páginasTRIPs & PatentsSunil YadavAinda não há avaliações
- Cohen Ill Ing WorthDocumento18 páginasCohen Ill Ing WorthManan PatelAinda não há avaliações
- Pharmaceutical Patenting in India: Problem of Public Access To HealthDocumento11 páginasPharmaceutical Patenting in India: Problem of Public Access To Health121933101040 VENKATA SAI RAMPELLIAinda não há avaliações
- Priority Sector Lending by Domestic Banks in LPG Market EnvironmentDocumento16 páginasPriority Sector Lending by Domestic Banks in LPG Market EnvironmentBalaji P NadarAinda não há avaliações
- Evolution of Designs Act in India & Protection of Industrial Designs Under International IPR RegimeDocumento17 páginasEvolution of Designs Act in India & Protection of Industrial Designs Under International IPR RegimeBalaji P Nadar88% (17)
- WTO Dispute Settlement Mechanism: A Critical AnalysisDocumento19 páginasWTO Dispute Settlement Mechanism: A Critical AnalysisBalaji P Nadar100% (5)
- CybersquattingDocumento23 páginasCybersquattingBalaji P NadarAinda não há avaliações
- Concept of Liberty: Its Emergence & EvolutionDocumento16 páginasConcept of Liberty: Its Emergence & EvolutionBalaji P Nadar100% (1)
- Comparative Study of Religious IndependenceDocumento18 páginasComparative Study of Religious IndependenceBalaji P NadarAinda não há avaliações
- Interview in Legal ResearchDocumento17 páginasInterview in Legal ResearchBalaji P Nadar100% (1)
- Doctrine of Pith and SubstanceDocumento16 páginasDoctrine of Pith and SubstanceBalaji P Nadar90% (20)
- Iomm VFD-3 030112Documento100 páginasIomm VFD-3 030112Alexander100% (1)
- SanMilan Inigo Cycling Physiology and Physiological TestingDocumento67 páginasSanMilan Inigo Cycling Physiology and Physiological Testingjesus.clemente.90Ainda não há avaliações
- Bio411 C1Documento1 páginaBio411 C1Aqiena BalqisAinda não há avaliações
- Brief RESUME EmailDocumento4 páginasBrief RESUME Emailranjit_kadalg2011Ainda não há avaliações
- Phardose Lab Prep 19 30Documento4 páginasPhardose Lab Prep 19 30POMPEYO BARROGAAinda não há avaliações
- Assignment - Lab Accidents and PrecautionsDocumento6 páginasAssignment - Lab Accidents and PrecautionsAnchu AvinashAinda não há avaliações
- Plica PDFDocumento7 páginasPlica PDFIVAN VERGARAAinda não há avaliações
- CBEU Service ConditionsDocumento623 páginasCBEU Service ConditionsAtul ModiAinda não há avaliações
- EXP 2 - Plug Flow Tubular ReactorDocumento18 páginasEXP 2 - Plug Flow Tubular ReactorOng Jia YeeAinda não há avaliações
- FINAL PAPER Marketing Plan For Rainbow Air PurifierDocumento12 páginasFINAL PAPER Marketing Plan For Rainbow Air PurifierMohola Tebello Griffith100% (1)
- Dressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionDocumento2 páginasDressmaking - Q1 TASK-SHEET v1 - Schalemar OmbionAlvaCatalinaAinda não há avaliações
- Recruitement Process - Siemens - Sneha Waman Kadam S200030047 PDFDocumento7 páginasRecruitement Process - Siemens - Sneha Waman Kadam S200030047 PDFSneha KadamAinda não há avaliações
- CONTROLTUB - Controle de Juntas - New-Flare-Piping-Joints-ControlDocumento109 páginasCONTROLTUB - Controle de Juntas - New-Flare-Piping-Joints-ControlVss SantosAinda não há avaliações
- Pantera 900Documento3 páginasPantera 900Tuan Pham AnhAinda não há avaliações
- 2133 Rla RlvaDocumento2 páginas2133 Rla RlvaAgung SubangunAinda não há avaliações
- Sav4747 PDFDocumento49 páginasSav4747 PDFAndres Antonio Moreno CastroAinda não há avaliações
- HVAC (Heating, Ventilation and Air Conditioning) : SRS PrecautionsDocumento1 páginaHVAC (Heating, Ventilation and Air Conditioning) : SRS PrecautionssoftallAinda não há avaliações
- Brody2012 PDFDocumento13 páginasBrody2012 PDFfrancisca caceresAinda não há avaliações
- Conference Version of SB 1Documento486 páginasConference Version of SB 1Paul MastersAinda não há avaliações
- Class Two Summer Vacation AssignmentDocumento1 páginaClass Two Summer Vacation AssignmentshahbazjamAinda não há avaliações
- BMJ 40 13Documento8 páginasBMJ 40 13Alvin JiwonoAinda não há avaliações
- Soalan 9 LainDocumento15 páginasSoalan 9 LainMelor DihatiAinda não há avaliações
- Case Report CMV RetinitisDocumento27 páginasCase Report CMV RetinitistaniamaulaniAinda não há avaliações
- University of Puerto Rico at PonceDocumento16 páginasUniversity of Puerto Rico at Ponceapi-583167359Ainda não há avaliações
- J130KDocumento6 páginasJ130KBelkisa ŠaćiriAinda não há avaliações
- Service Bulletins For Engine Model I0360kb.3Documento6 páginasService Bulletins For Engine Model I0360kb.3Randy Johel Cova FlórezAinda não há avaliações
- DPA Fact Sheet Women Prison and Drug War Jan2015 PDFDocumento2 páginasDPA Fact Sheet Women Prison and Drug War Jan2015 PDFwebmaster@drugpolicy.orgAinda não há avaliações
- MajorProjects 202112 e 1Documento64 páginasMajorProjects 202112 e 1xtrooz abiAinda não há avaliações
- SPA - MichaelDocumento1 páginaSPA - Michaelgilberthufana446877Ainda não há avaliações
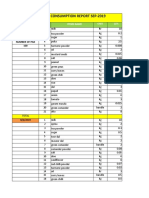
- Daily Staff Food Consumption Reports Sep-2019Documento4 páginasDaily Staff Food Consumption Reports Sep-2019Manjit RawatAinda não há avaliações