Você também pode gostar
- Cath Lab Cardiac Cath LabDocumento3 páginasCath Lab Cardiac Cath LabMaria Edel100% (2)
- Validation Master PlanDocumento27 páginasValidation Master PlanPrashansa Shrestha85% (13)
- Dr. M's CPT Study GuideDocumento10 páginasDr. M's CPT Study GuideKalah EdmersonAinda não há avaliações
- Heart Lung MachineDocumento3 páginasHeart Lung MachinerythmicinAinda não há avaliações
- Atsp Book 2011Documento24 páginasAtsp Book 2011Chengyuan ZhangAinda não há avaliações
- House Designs, QHC, 1950Documento50 páginasHouse Designs, QHC, 1950House Histories100% (8)
- Pain Audit ToolsDocumento10 páginasPain Audit ToolsIrmela CoricAinda não há avaliações
- Effective Time ManagementDocumento61 páginasEffective Time ManagementTafadzwa94% (16)
- Sinus ArrhythmiaDocumento6 páginasSinus ArrhythmiaVincent Maralit MaterialAinda não há avaliações
- Apollo TyresDocumento78 páginasApollo TyresADITYA33% (3)
- Aircraft Design Project 2Documento80 páginasAircraft Design Project 2Technology Informer90% (21)
- Manual Emergency Revise EdditionDocumento264 páginasManual Emergency Revise Edditionshahidchaudhary100% (5)
- SBAR WorksheetDocumento3 páginasSBAR Worksheet6bigstar9Ainda não há avaliações
- 29744226: Cerebral Pathophysiology in Extracorporeal Membrane Oxygenation Pitfalls in Daily Clinical ManagementDocumento11 páginas29744226: Cerebral Pathophysiology in Extracorporeal Membrane Oxygenation Pitfalls in Daily Clinical ManagementEward Rod SalAinda não há avaliações
- Medical-Surgical Nursing Review Flashcards - QuizletDocumento14 páginasMedical-Surgical Nursing Review Flashcards - QuizletNursyNurse100% (1)
- Space DynamicsDocumento37 páginasSpace Dynamicspurushottam KashyapAinda não há avaliações
- The Temple of ChaosDocumento43 páginasThe Temple of ChaosGauthier GohorryAinda não há avaliações
- Thermal BurnsDocumento50 páginasThermal BurnsPooya WindyAinda não há avaliações
- Theoretical and Actual CombustionDocumento14 páginasTheoretical and Actual CombustionErma Sulistyo R100% (1)
- Hospital Incident ReportingDocumento32 páginasHospital Incident Reportingakhtarulmunim2279Ainda não há avaliações
- Blood Transfusion Reactions: Life Saving Yet Life ThreateningDocumento52 páginasBlood Transfusion Reactions: Life Saving Yet Life Threateninganam farzand100% (2)
- Chapter 5: Analyzing A Rhythm StripDocumento7 páginasChapter 5: Analyzing A Rhythm StriptellyAinda não há avaliações
- Draft Blood Bank Standards Seek Feedback by June 30thDocumento101 páginasDraft Blood Bank Standards Seek Feedback by June 30thGagan DudejaAinda não há avaliações
- Management of The EVDDocumento7 páginasManagement of The EVDplethoraldork100% (1)
- GIS AccidentsDocumento5 páginasGIS Accidentsali110011Ainda não há avaliações
- Orientation Booklet For ED PhysicianDocumento10 páginasOrientation Booklet For ED PhysicianshahidchaudharyAinda não há avaliações
- Safe Injection Practices and Handling of SharpsDocumento26 páginasSafe Injection Practices and Handling of SharpsbrightyAinda não há avaliações
- Percutaneous Coronary Intervention 10 05Documento8 páginasPercutaneous Coronary Intervention 10 05benypermadiAinda não há avaliações
- Pre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIDocumento25 páginasPre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIFatima MAinda não há avaliações
- 2012 Cath Lab Consensus DocumentDocumento85 páginas2012 Cath Lab Consensus DocumentDorin DocAinda não há avaliações
- Emergency Dept Plan 2016Documento16 páginasEmergency Dept Plan 2016shahidchaudharyAinda não há avaliações
- Dialysis Technician Seeking Clinical RoleDocumento4 páginasDialysis Technician Seeking Clinical RoleGloria Jaison100% (1)
- Weaning From Mechanical Ventilation Using SBT PDFDocumento29 páginasWeaning From Mechanical Ventilation Using SBT PDFEdgar Bravo Santibañez100% (1)
- Plasmapheresis Procedure Removes Antibodies From BloodstreamDocumento13 páginasPlasmapheresis Procedure Removes Antibodies From BloodstreamSampath GoudAinda não há avaliações
- Access For Dialysis - Surgical and Radiologic ProceduresDocumento436 páginasAccess For Dialysis - Surgical and Radiologic ProceduresAriadna Mariniuc100% (1)
- Nursing Audit Tool PDFDocumento12 páginasNursing Audit Tool PDFjamieAinda não há avaliações
- Cardioplegia Types and Methods of AdministrationDocumento57 páginasCardioplegia Types and Methods of Administrationgovind_soni_15Ainda não há avaliações
- Scripps Hospital Patient Visitor Policy PDFDocumento2 páginasScripps Hospital Patient Visitor Policy PDFcode4saleAinda não há avaliações
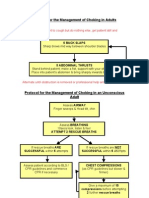
- Protocol For The Management of Choking in AdultsDocumento3 páginasProtocol For The Management of Choking in AdultsSarinah RynaAinda não há avaliações
- Nursing Diagnoses Arranged by GordonDocumento9 páginasNursing Diagnoses Arranged by GordonJoedeson Aroco BungubungAinda não há avaliações
- CIRC 314-AN 178 INP EN EDENPROD 195309 v1Documento34 páginasCIRC 314-AN 178 INP EN EDENPROD 195309 v1xloriki_100% (1)
- TB QuestionnaireDocumento1 páginaTB QuestionnaireaplesgjskAinda não há avaliações
- Hyperthermic Intraperitoneal Chemotherapy - Hipec-: Rusie Daniel, Medic Rezident Chirurgie GeneralaDocumento23 páginasHyperthermic Intraperitoneal Chemotherapy - Hipec-: Rusie Daniel, Medic Rezident Chirurgie GeneralaDaniel RusieAinda não há avaliações
- Guidelines On The Use of CRS and HIPEC PDFDocumento13 páginasGuidelines On The Use of CRS and HIPEC PDFAyunda Shinta NurarliahAinda não há avaliações
- KDIGO 2012 Clinical Practice Guideline for the Prevention, Detection, Evaluation and Management of Acute Kidney InjuryDocumento40 páginasKDIGO 2012 Clinical Practice Guideline for the Prevention, Detection, Evaluation and Management of Acute Kidney InjuryAbedDabajaAinda não há avaliações
- Guide to Measuring Vital SignsDocumento32 páginasGuide to Measuring Vital SignsJacqueline de AsisAinda não há avaliações
- Module 9 Mechanical Ventilation PDFDocumento46 páginasModule 9 Mechanical Ventilation PDFChabboo SutabrataAinda não há avaliações
- Role of Food and Its Medicinal ValueDocumento9 páginasRole of Food and Its Medicinal Valueharshika tembhurneAinda não há avaliações
- EKGTechnician 50hours 5 4 05Documento1 páginaEKGTechnician 50hours 5 4 05ledarius_c114Ainda não há avaliações
- Heart-Lung MachineDocumento4 páginasHeart-Lung Machinearsalanbook100% (2)
- Advanced Airway Care: Intensive Care Unit PerspectiveDocumento42 páginasAdvanced Airway Care: Intensive Care Unit PerspectiveJeffery Samuel100% (1)
- Citrate Protocol 2020Documento5 páginasCitrate Protocol 2020Katrina Mae AntalanAinda não há avaliações
- CPG Management of Percutaneous Coronory Intervention (PCI) 2009Documento92 páginasCPG Management of Percutaneous Coronory Intervention (PCI) 2009umiraihana1Ainda não há avaliações
- Management of Arterial LineDocumento16 páginasManagement of Arterial LineFarcasanu Liana GeorgianaAinda não há avaliações
- Acute Nutrition PolicyDocumento79 páginasAcute Nutrition PolicyyohaneskoAinda não há avaliações
- Clinical Science Questions and Answers - Standards MaintainedDocumento7 páginasClinical Science Questions and Answers - Standards MaintainedManish JainAinda não há avaliações
- 5 Shock PPT EnglishDocumento77 páginas5 Shock PPT EnglishKessi VikaneswariAinda não há avaliações
- Critical Care 2012Documento490 páginasCritical Care 2012Carlos PradoAinda não há avaliações
- 17 Intensive CareDocumento6 páginas17 Intensive CareEmad ElhusseinAinda não há avaliações
- Missing Persons Policy SummaryDocumento16 páginasMissing Persons Policy SummaryAgnieszka WaligóraAinda não há avaliações
- Blood Transfusion Single Use PathwayDocumento6 páginasBlood Transfusion Single Use PathwayropusanAinda não há avaliações
- Invasive Devices On CXRDocumento1 páginaInvasive Devices On CXRLaurensia Erlina NataliaAinda não há avaliações
- Vascular Acess Number 1Documento45 páginasVascular Acess Number 1Paulo GalangAinda não há avaliações
- Drug Compliance Among Hypertensive PatientsDocumento5 páginasDrug Compliance Among Hypertensive PatientsSyifa MunawarahAinda não há avaliações
- Critical Care Skills Checklist: Personal InformationDocumento5 páginasCritical Care Skills Checklist: Personal InformationRin noharaAinda não há avaliações
- Cardiac MonitorDocumento4 páginasCardiac MonitorFahyesha MaulaniAinda não há avaliações
- Ed Assessment Tool SampleDocumento28 páginasEd Assessment Tool SampleAnonymous ibmeej9Ainda não há avaliações
- Anesthesia and ResuscitationDocumento24 páginasAnesthesia and ResuscitationaviabiAinda não há avaliações
- Scape Vs FospeDocumento5 páginasScape Vs FospeDr. FarhanAinda não há avaliações
- DVT Assessment FormDocumento1 páginaDVT Assessment FormLoy ZiAinda não há avaliações
- Icu Sop: TOPIC: Length of Stay in ICUDocumento5 páginasIcu Sop: TOPIC: Length of Stay in ICURohit RajeevanAinda não há avaliações
- ICU Scoring Systems A Complete Guide - 2020 EditionNo EverandICU Scoring Systems A Complete Guide - 2020 EditionAinda não há avaliações
- Hamā Anjuman Prayers For Naurooz in English, Farsi and GujaratiDocumento52 páginasHamā Anjuman Prayers For Naurooz in English, Farsi and Gujaratiismail_radAinda não há avaliações
- What Is ResearchDocumento4 páginasWhat Is ResearchshahidchaudharyAinda não há avaliações
- What Was The Age of Ummul MomininDocumento8 páginasWhat Was The Age of Ummul MomininshahidchaudharyAinda não há avaliações
- Wife Beating in Islam? The Quran Strikes Back!Documento43 páginasWife Beating in Islam? The Quran Strikes Back!TruthResearcher100% (1)
- RibaDocumento68 páginasRibashahidchaudharyAinda não há avaliações
- Misbha Al SalatDocumento83 páginasMisbha Al SalatshahidchaudharyAinda não há avaliações
- Bivi PR Tashadad Ghair Qurani HeyDocumento16 páginasBivi PR Tashadad Ghair Qurani HeyshahidchaudharyAinda não há avaliações
- Qibla Aor Bait Al MaqdasDocumento4 páginasQibla Aor Bait Al MaqdasshahidchaudharyAinda não há avaliações
- Quran Ki TafheemDocumento39 páginasQuran Ki TafheemshahidchaudharyAinda não há avaliações
- Momin Ki NamazDocumento55 páginasMomin Ki NamazshahidchaudharyAinda não há avaliações
- Salat Interpreted WrongDocumento7 páginasSalat Interpreted WrongshahidchaudharyAinda não há avaliações
- Respect of Ahle Bait in Eye of Ahle Sunna Wal JumaatDocumento24 páginasRespect of Ahle Bait in Eye of Ahle Sunna Wal JumaatshahidchaudharyAinda não há avaliações
- Characteristics of Prophet Muhammad (MPUH) in Torah and BibleDocumento11 páginasCharacteristics of Prophet Muhammad (MPUH) in Torah and BibleshahidchaudharyAinda não há avaliações
- TauheedDocumento158 páginasTauheedshahidchaudharyAinda não há avaliações
- Wrong Interpretation of Hadiets To SupportDocumento4 páginasWrong Interpretation of Hadiets To SupportshahidchaudharyAinda não há avaliações
- Tubah King of Yaman and His Believe On Muhommad AslatowaslamDocumento10 páginasTubah King of Yaman and His Believe On Muhommad AslatowaslamshahidchaudharyAinda não há avaliações
- Attanding The Roza Rasool With Respect and Is PermissableDocumento13 páginasAttanding The Roza Rasool With Respect and Is PermissableshahidchaudharyAinda não há avaliações
- Hadiths of Prophet Muhammad (Aslatowaslam)Documento180 páginasHadiths of Prophet Muhammad (Aslatowaslam)shahidchaudharyAinda não há avaliações
- A Study of Primary Health Care Referrals in Qaseem Region Saudi ArabDocumento8 páginasA Study of Primary Health Care Referrals in Qaseem Region Saudi ArabshahidchaudharyAinda não há avaliações
- Orientation Booklet For Emergency DepartmentDocumento10 páginasOrientation Booklet For Emergency Departmentshahidchaudhary100% (1)
- DO NOT RESUSCITATE (DNR) BY DR Shahid Bashir ChaudharyDocumento2 páginasDO NOT RESUSCITATE (DNR) BY DR Shahid Bashir ChaudharyshahidchaudharyAinda não há avaliações
- Emergency Department Staffing PlanDocumento5 páginasEmergency Department Staffing PlanshahidchaudharyAinda não há avaliações
- WK 43 - Half-Past-TwoDocumento2 páginasWK 43 - Half-Past-TwoKulin RanaweeraAinda não há avaliações
- Flood FillDocumento1 páginaFlood FillshubhamAinda não há avaliações
- SOR 8th Ed 2013Documento467 páginasSOR 8th Ed 2013Durgesh Govil100% (3)
- Is.4162.1.1985 Graduated PipettesDocumento23 páginasIs.4162.1.1985 Graduated PipettesBala MuruAinda não há avaliações
- Are Hypomineralized Primary Molars and Canines Associated With Molar-Incisor HypomineralizationDocumento5 páginasAre Hypomineralized Primary Molars and Canines Associated With Molar-Incisor HypomineralizationDr Chevyndra100% (1)
- Transport of OxygenDocumento13 páginasTransport of OxygenSiti Nurkhaulah JamaluddinAinda não há avaliações
- Metal Framing SystemDocumento56 páginasMetal Framing SystemNal MénAinda não há avaliações
- Usjr Temfacil Balance of Work Schedule Aug 25, 2022Documento5 páginasUsjr Temfacil Balance of Work Schedule Aug 25, 2022Maribeth PalumarAinda não há avaliações
- F-16c.1 Ginkgo Ginkgolic AcidDocumento2 páginasF-16c.1 Ginkgo Ginkgolic AcidNarongchai PongpanAinda não há avaliações
- Direct From: 1St Quarter 2020Documento23 páginasDirect From: 1St Quarter 2020JeanAinda não há avaliações
- Front Wheel Steering System With Movable Hedlights Ijariie5360Documento6 páginasFront Wheel Steering System With Movable Hedlights Ijariie5360Ifra KhanAinda não há avaliações
- WOOD Investor Presentation 3Q21Documento65 páginasWOOD Investor Presentation 3Q21Koko HadiwanaAinda não há avaliações
- Chap06 (6 24 06)Documento74 páginasChap06 (6 24 06)pumba1234Ainda não há avaliações
- Embankment PDFDocumento5 páginasEmbankment PDFTin Win HtutAinda não há avaliações
- 07.03.09 Chest Physiotherapy PDFDocumento9 páginas07.03.09 Chest Physiotherapy PDFRakesh KumarAinda não há avaliações
- Detection and Attribution Methodologies Overview: Appendix CDocumento9 páginasDetection and Attribution Methodologies Overview: Appendix CDinesh GaikwadAinda não há avaliações
- Phenomenological of in Church and TV WorshipDocumento18 páginasPhenomenological of in Church and TV WorshipCindy TirtaAinda não há avaliações
- Introduction To Finite Element Methods (2001) (En) (489s)Documento489 páginasIntroduction To Finite Element Methods (2001) (En) (489s)green77parkAinda não há avaliações
- Oecumenius’ Exegetical Method in His Commentary on the RevelationDocumento10 páginasOecumenius’ Exegetical Method in His Commentary on the RevelationMichał WojciechowskiAinda não há avaliações