Você também pode gostar
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsNo EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsNota: 5 de 5 estrelas5/5 (9)
- Taxation One Complete Updated (Atty. Mickey Ingles)Documento116 páginasTaxation One Complete Updated (Atty. Mickey Ingles)Patty Salas - Padua100% (11)
- z30tq Pediatric Nutrition Handbook 6th EditionDocumento52 páginasz30tq Pediatric Nutrition Handbook 6th EditionJair OsorioAinda não há avaliações
- Epi PowerpointDocumento29 páginasEpi PowerpointFelisa Lacsamana Gregorio100% (3)
- Clinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3No EverandClinical Management Review 2023-2024: Volume 1: USMLE Step 3 and COMLEX-USA Level 3Nota: 5 de 5 estrelas5/5 (1)
- How To Make Papaya SoapDocumento10 páginasHow To Make Papaya SoapEmz GamboaAinda não há avaliações
- Lesson Plan 4Documento6 páginasLesson Plan 4Lilay Barambangan100% (3)
- Catherine Davies - Modernity, Masculinity, and Imperfect Cinema in CubaDocumento16 páginasCatherine Davies - Modernity, Masculinity, and Imperfect Cinema in CubakahlilchaarAinda não há avaliações
- Vacunas 2012Documento7 páginasVacunas 2012dr.alexisleon9124Ainda não há avaliações
- Adult Immunization ScheduleDocumento3 páginasAdult Immunization ScheduleBryan Mae H. DegorioAinda não há avaliações
- Adult ScheduleDocumento3 páginasAdult ScheduledrmanojvimalAinda não há avaliações
- Adult Combined ScheduleDocumento5 páginasAdult Combined SchedulelcmurilloAinda não há avaliações
- Adult Combined ScheduleDocumento5 páginasAdult Combined ScheduleAwal Safar MAinda não há avaliações
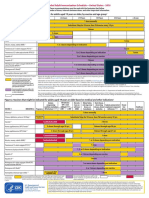
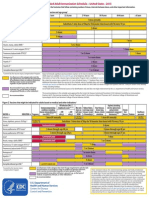
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocumento2 páginasFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasAinda não há avaliações
- Adult Pocafeket SizeDocumento2 páginasAdult Pocafeket SizedadfAinda não há avaliações
- Clinical Guideline: Recommended Adult Immunization Schedule: United States, 2011Documento8 páginasClinical Guideline: Recommended Adult Immunization Schedule: United States, 2011Hery PriyantoAinda não há avaliações
- Your Child's Best Defense: ImmunizationsDocumento2 páginasYour Child's Best Defense: ImmunizationsNoble ChunAinda não há avaliações
- ScheduleDocumento2 páginasScheduleapi-286634335Ainda não há avaliações
- Immunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaDocumento24 páginasImmunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaEugene YeboahAinda não há avaliações
- Adult ScheduleDocumento3 páginasAdult SchedulelcmurilloAinda não há avaliações
- Piis0025619619305737 220530 065558Documento11 páginasPiis0025619619305737 220530 065558Garcia Yepez Stephanie GraceAinda não há avaliações
- MMWR HiB PDFDocumento20 páginasMMWR HiB PDFworksheetbookAinda não há avaliações
- Splenectomy: DisclaimerDocumento5 páginasSplenectomy: DisclaimerMimi FatinAinda não há avaliações
- Months After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18Documento11 páginasMonths After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18api-30279712Ainda não há avaliações
- Pneumococcal Conjugate: VaccineDocumento2 páginasPneumococcal Conjugate: VaccineJenny TaylorAinda não há avaliações
- Adult Schedule 11x17Documento2 páginasAdult Schedule 11x17lcmurilloAinda não há avaliações
- ImmunizationsDocumento2 páginasImmunizationsSonny KusumaAinda não há avaliações
- Pediatrics 2012 780 92Documento15 páginasPediatrics 2012 780 92ERICKAinda não há avaliações
- Research Paper On Childhood VaccinationsDocumento8 páginasResearch Paper On Childhood Vaccinationsefjr9yx3100% (1)
- Peds 2011-1330 FullDocumento18 páginasPeds 2011-1330 FullbealacambraAinda não há avaliações
- Immunization in The United States: Recommendations, Barriers, and Measures To Improve ComplianceDocumento2 páginasImmunization in The United States: Recommendations, Barriers, and Measures To Improve CompliancecaaarleeyAinda não há avaliações
- Pneumonia in Infants and ChildrenDocumento52 páginasPneumonia in Infants and ChildrenMikeyAinda não há avaliações
- PPS-PIDSP Joint Position Statement On COVID-19 VaccinationDocumento3 páginasPPS-PIDSP Joint Position Statement On COVID-19 VaccinationCae OnghansengAinda não há avaliações
- Diagnosis/vaccination/: Hepatitis B VaccineDocumento6 páginasDiagnosis/vaccination/: Hepatitis B Vaccinereza satriaAinda não há avaliações
- Epi NotesDocumento5 páginasEpi NoteshoneykrizelAinda não há avaliações
- Undernutrition Among HIV-positive Children of Age 1-5 Years Attending The ART Clinic in Bushenyi Health Centre IV Ishaka-Bushenyi Municipality, Bushenyi DistrictDocumento9 páginasUndernutrition Among HIV-positive Children of Age 1-5 Years Attending The ART Clinic in Bushenyi Health Centre IV Ishaka-Bushenyi Municipality, Bushenyi DistrictKIU PUBLICATION AND EXTENSIONAinda não há avaliações
- Retraction-Ileal-lymphoid-nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocumento1 páginaRetraction-Ileal-lymphoid-nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenOutlawHealthAinda não há avaliações
- Pediatrics 2014 Queen E23 9Documento10 páginasPediatrics 2014 Queen E23 9Desrainy InhardiniAinda não há avaliações
- Moderately Affected Children Tonsillectomy and Adenotonsillectomy For Recurrent Throat Infection inDocumento11 páginasModerately Affected Children Tonsillectomy and Adenotonsillectomy For Recurrent Throat Infection inKarlina MiaowAinda não há avaliações
- Pertussis VaccinesDocumento7 páginasPertussis VaccinesNur SulistiyaningsihAinda não há avaliações
- Moderately Affected Children Tonsillectomy and Adenotonsillectomy For Recurrent Throat Infection inDocumento11 páginasModerately Affected Children Tonsillectomy and Adenotonsillectomy For Recurrent Throat Infection inReza Rizky Al RasyidAinda não há avaliações
- PediatricguidelinesDocumento333 páginasPediatricguidelinespradeep36Ainda não há avaliações
- Community Health Nursing (Learning Feedback Diary (LFD #25)Documento3 páginasCommunity Health Nursing (Learning Feedback Diary (LFD #25)Angelica Malacay RevilAinda não há avaliações
- Pediatrics 2013 E1089 104Documento18 páginasPediatrics 2013 E1089 104phobicmdAinda não há avaliações
- Rotaviruses Diarrhea: What Are The Benefits of The Rotavirus Vaccine?Documento5 páginasRotaviruses Diarrhea: What Are The Benefits of The Rotavirus Vaccine?Mikko ArriesgoddessAinda não há avaliações
- Literature Review On Childhood ImmunizationDocumento4 páginasLiterature Review On Childhood Immunizationc5e4jfpn100% (1)
- 2011 Ispad NeumoníaDocumento14 páginas2011 Ispad NeumoníaAaron Nureña JaraAinda não há avaliações
- Recommended Childhood and Adolescent Immunization Schedule: United States, 2020Documento5 páginasRecommended Childhood and Adolescent Immunization Schedule: United States, 2020nanaAinda não há avaliações
- Shots For This Fall and WinterDocumento7 páginasShots For This Fall and WinterRosario Ordoñez NavaAinda não há avaliações
- Pneumonia Comparative Effectiveness of Empiric Antibiotics For Community-AcquiredDocumento9 páginasPneumonia Comparative Effectiveness of Empiric Antibiotics For Community-AcquiredSulis Na EndutzAinda não há avaliações
- Recommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Documento2 páginasRecommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Maja MudriAinda não há avaliações
- Reading VaccineImmunizationDocumento13 páginasReading VaccineImmunizationelztly4694Ainda não há avaliações
- Jurnal 1Documento7 páginasJurnal 1Deski MadeAinda não há avaliações
- Oma - Aap 2012Documento38 páginasOma - Aap 2012yosiaputraAinda não há avaliações
- Ijerph 17 03694Documento13 páginasIjerph 17 03694Ana-Maria CiobotaruAinda não há avaliações
- Nej Mo JurnalDocumento11 páginasNej Mo JurnalAnnisa RahmaniAinda não há avaliações
- CHN 1 LEC WEEK 9 Records in Family Health Nursing PracticeDocumento14 páginasCHN 1 LEC WEEK 9 Records in Family Health Nursing PracticeSenyorita ArdiAinda não há avaliações
- Cir 531Documento52 páginasCir 531Nubia PuAinda não há avaliações
- Vaccines - The Week in Review - 3 January 2011Documento16 páginasVaccines - The Week in Review - 3 January 2011davidrcurryAinda não há avaliações
- Cir 531Documento52 páginasCir 531Mario CornejoAinda não há avaliações
- Nac Idsa PDFDocumento52 páginasNac Idsa PDFYULIETH ANDREA SAAVEDRA COGOLLOAinda não há avaliações
- Deb Week 8 Discussion - EditedDocumento7 páginasDeb Week 8 Discussion - Editeddominic hoganAinda não há avaliações
- 2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisDocumento22 páginas2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisAuliaRahmanAinda não há avaliações
- NAC en NiñosDocumento14 páginasNAC en NiñosAnonymous DxJyWJwtAinda não há avaliações
- Moatiz Riaz - Area Sales ManagerDocumento1 páginaMoatiz Riaz - Area Sales ManagerMoatiz RiazAinda não há avaliações
- Sistem Informasi Pencatatan Data Pelanggan Pada Telkomsel Grapari Banda AcehDocumento6 páginasSistem Informasi Pencatatan Data Pelanggan Pada Telkomsel Grapari Banda AcehJurnal JTIK (Jurnal Teknologi Informasi dan Komunikasi)Ainda não há avaliações
- Buyer Behavior ModelDocumento1 páginaBuyer Behavior ModelraihanulhasanAinda não há avaliações
- Essentials of Materials Science and Engineering Si Edition 3rd Edition Askeland Solutions ManualDocumento11 páginasEssentials of Materials Science and Engineering Si Edition 3rd Edition Askeland Solutions Manualjeffreyhayesagoisypdfm100% (13)
- Different Strategies in TeachingDocumento12 páginasDifferent Strategies in TeachingCris MolinaAinda não há avaliações
- Midterm Test 1Documento3 páginasMidterm Test 1Hùng Trường NguyễnAinda não há avaliações
- TaxationDocumento26 páginasTaxationReynamae Garcia AbalesAinda não há avaliações
- Class 11 Assignment 10 (Prac)Documento3 páginasClass 11 Assignment 10 (Prac)9crollno14bhewensagarsahuAinda não há avaliações
- Jeevan Tara, Sansad Marg NEW DELHI-11001 Regonal Office (North Zone) E MailDocumento3 páginasJeevan Tara, Sansad Marg NEW DELHI-11001 Regonal Office (North Zone) E MailGourav SharmaAinda não há avaliações
- Milling Machine Maintenance, Safety and OperationDocumento3 páginasMilling Machine Maintenance, Safety and OperationPPSwain100% (1)
- Project Proposal Environmental Protection Program-DeNRDocumento57 páginasProject Proposal Environmental Protection Program-DeNRLGU PadadaAinda não há avaliações
- Natural Gas DistributionDocumento46 páginasNatural Gas DistributionscribdmisraAinda não há avaliações
- 1.4 Creating Graphic OrganizerDocumento1 página1.4 Creating Graphic OrganizerTrixie Roselle Y. MesiasAinda não há avaliações
- Case Study of AmoebiasisDocumento16 páginasCase Study of AmoebiasisGlorielle ElvambuenaAinda não há avaliações
- E5170s-22 LTE CPE - Quick Start Guide - 01 - English - ErP - C - LDocumento24 páginasE5170s-22 LTE CPE - Quick Start Guide - 01 - English - ErP - C - LNelsonAinda não há avaliações
- How To Read Research PaperDocumento7 páginasHow To Read Research Papertuigauund100% (1)
- Internship Proposal FormDocumento3 páginasInternship Proposal FormMuhammad FidaAinda não há avaliações
- Global Perspectives Reflective PaperDocumento3 páginasGlobal Perspectives Reflective PaperMoaiz AttiqAinda não há avaliações
- INSTRUCTIONS FOR USOL PRIVATE REAPPEAR DE January 2022Documento4 páginasINSTRUCTIONS FOR USOL PRIVATE REAPPEAR DE January 2022RaghavAinda não há avaliações
- The Case For A Concentrated Portfolio 6-30-16Documento4 páginasThe Case For A Concentrated Portfolio 6-30-16Maria Gabriela PopaAinda não há avaliações
- Satellite Motion NotesDocumento23 páginasSatellite Motion NotesVarshLok100% (1)
- Zimbabwe National Code Ccorporate GovernanceDocumento96 páginasZimbabwe National Code Ccorporate GovernanceHerbert NgwaraiAinda não há avaliações
- Bcos 186Documento3 páginasBcos 186Shiv KumarAinda não há avaliações
- Maha Nirvana Tantra EngDocumento200 páginasMaha Nirvana Tantra EngDev Vyas100% (2)
- Chapter 1Documento38 páginasChapter 1Kurt dela Torre100% (1)
- Chapter 3 ContDocumento12 páginasChapter 3 ContVenus Frias-AntonioAinda não há avaliações