Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- PTFE HZ-2 HoerbigerDocumento2 páginasPTFE HZ-2 HoerbigerТатьяна ВасильеваAinda não há avaliações
- Street Design Manual NYCDocumento312 páginasStreet Design Manual NYCgonleoAinda não há avaliações
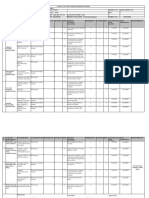
- Factory Program Library List v1.0Documento9 páginasFactory Program Library List v1.0Ronaldo DamattaAinda não há avaliações
- Abnormal Uterine Bleeding - Surgical ManagementDocumento14 páginasAbnormal Uterine Bleeding - Surgical ManagementNikhil DevAinda não há avaliações
- WST Macros Add-In FeaturesDocumento1 páginaWST Macros Add-In FeaturesTrader CatAinda não há avaliações
- Wheatley Hp600 Quintuplex Plunger PumpDocumento2 páginasWheatley Hp600 Quintuplex Plunger Pumpmetasoniko2014Ainda não há avaliações
- HorticultureDocumento12 páginasHorticultureवरुण राठीAinda não há avaliações
- ELK-3 550 1HC0000742AFEnDocumento20 páginasELK-3 550 1HC0000742AFEnOnur FişekAinda não há avaliações
- Nursing Practice Skills: Adult Intensive Care Unit PatientsDocumento10 páginasNursing Practice Skills: Adult Intensive Care Unit PatientsMona Doria67% (3)
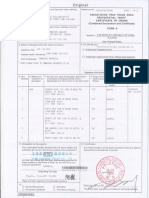
- Form 03B Heritage Bell 1Documento2 páginasForm 03B Heritage Bell 1ValAinda não há avaliações
- Hinomoto Tractor Parts Catalogue 2018 C144, C174, E150, E180, E230, E250, E280, E384Documento63 páginasHinomoto Tractor Parts Catalogue 2018 C144, C174, E150, E180, E230, E250, E280, E384Monica Mascarenhas0% (1)
- Hira - For Shot Blasting & Upto 2nd Coat of PaintingDocumento15 páginasHira - For Shot Blasting & Upto 2nd Coat of PaintingDhaneswar SwainAinda não há avaliações
- Therelek - Heat Treatment ServicesDocumento8 páginasTherelek - Heat Treatment ServicesTherelek EngineersAinda não há avaliações
- Dense Ball PackingDocumento334 páginasDense Ball PackingLucas RibeiroAinda não há avaliações
- Ref Manual - Additives For MA Spinel PDFDocumento5 páginasRef Manual - Additives For MA Spinel PDFRITWIK SARKARAinda não há avaliações
- Masterseal 530: Surface Applied Capillary Waterproofing For Concrete and MortarDocumento2 páginasMasterseal 530: Surface Applied Capillary Waterproofing For Concrete and MortarHoang An ViAinda não há avaliações
- TMJDocumento38 páginasTMJAnonymous 6kAmeZzIAinda não há avaliações
- Listening DictationDocumento3 páginasListening DictationThảo ĐinhAinda não há avaliações
- Manual de Servico Samsung Sgh-I677-Eplis-11Documento10 páginasManual de Servico Samsung Sgh-I677-Eplis-11Anselmo Antunes0% (1)
- Architect As An Environmental PlannerDocumento14 páginasArchitect As An Environmental PlannerJames Adrian MoralAinda não há avaliações
- Aviation MagazinesDocumento46 páginasAviation Magazinesyogaga100% (1)
- Chapter-01 Introduction: Sonadanga Residential Area (1st Phase)Documento17 páginasChapter-01 Introduction: Sonadanga Residential Area (1st Phase)MAFRID HAYDARAinda não há avaliações
- 9trffi&hpr.! Ni-: Use E EDocumento2 páginas9trffi&hpr.! Ni-: Use E ERafi ZulfiAinda não há avaliações
- Carpentry 7&8 Quarter 4-Module 1.2Documento8 páginasCarpentry 7&8 Quarter 4-Module 1.2Mark Laurence EchaluceAinda não há avaliações
- REM Geo&Man Comp 2016Documento350 páginasREM Geo&Man Comp 2016youungAinda não há avaliações
- Dobdsm 304Documento39 páginasDobdsm 304LuisangelDueñasAinda não há avaliações
- Compressed Air Pressure Drop DiagramDocumento4 páginasCompressed Air Pressure Drop DiagramycemalAinda não há avaliações
- Nfpa 13d 2007 IndexDocumento3 páginasNfpa 13d 2007 Indexsaladin1977Ainda não há avaliações
- 10 de Thi Tieng Anh Hướng Dẫn Giải Chi TiếtDocumento145 páginas10 de Thi Tieng Anh Hướng Dẫn Giải Chi TiếtVuong DiepAinda não há avaliações
- STAN Statistika 12 PDFDocumento25 páginasSTAN Statistika 12 PDFPembelajaran Jarak JauhAinda não há avaliações