Você também pode gostar
- Recognizing The Burden of Injuries in PakistanDocumento4 páginasRecognizing The Burden of Injuries in PakistanSabeenaJalalAinda não há avaliações
- An Ethnographic Look at The Status of Health of Women Living in An Urban Squatter Settlement of Karachi.Documento17 páginasAn Ethnographic Look at The Status of Health of Women Living in An Urban Squatter Settlement of Karachi.SabeenaJalalAinda não há avaliações
- Trauma Talk in A Developing WorldDocumento2 páginasTrauma Talk in A Developing WorldSabeenaJalalAinda não há avaliações
- UntitledDocumento2 páginasUntitledSabeenaJalal100% (1)
- Sports Medicine: A Neglected Field in A Developing CountryDocumento3 páginasSports Medicine: A Neglected Field in A Developing CountrySabeenaJalalAinda não há avaliações
- Sports Medicine: A Neglected Field in A Developing Country. (Article Was Publis Hed in 2007)Documento1 páginaSports Medicine: A Neglected Field in A Developing Country. (Article Was Publis Hed in 2007)SabeenaJalalAinda não há avaliações
- Scared To ScreamDocumento3 páginasScared To ScreamSabeenaJalalAinda não há avaliações
- Trauma CentreDocumento2 páginasTrauma CentreSabeenaJalalAinda não há avaliações
- Diagnosis of Enteric Fever in The Emergency Department of Pakistan. Ali Faisal SaleemDocumento5 páginasDiagnosis of Enteric Fever in The Emergency Department of Pakistan. Ali Faisal SaleemAli Faisal SaleemAinda não há avaliações
- The Suffering ContinuesDocumento4 páginasThe Suffering ContinuesSabeenaJalalAinda não há avaliações
- FLOOD 2010 PAKISTAN RELATED ARTICLE # 1: Disaster Mitigation - A Coordinated Effort Model. by Sabeena Jalal and Shahzad Ali KhanDocumento3 páginasFLOOD 2010 PAKISTAN RELATED ARTICLE # 1: Disaster Mitigation - A Coordinated Effort Model. by Sabeena Jalal and Shahzad Ali KhanSabeenaJalalAinda não há avaliações
- Working From HomeDocumento3 páginasWorking From HomeSabeenaJalalAinda não há avaliações
- IPV - Italian Journal of Public HealthDocumento3 páginasIPV - Italian Journal of Public HealthSabeenaJalalAinda não há avaliações
- GisDocumento4 páginasGisSabeenaJalalAinda não há avaliações
- GisDocumento4 páginasGisSabeenaJalalAinda não há avaliações
- Awareness About DiseasesDocumento4 páginasAwareness About DiseasesSabeenaJalalAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- CHEMISTRY (CY11003) : Autumn 2021 - 2022Documento15 páginasCHEMISTRY (CY11003) : Autumn 2021 - 2022Ashish RanjanAinda não há avaliações
- Vinyl Strip FlooringDocumento2 páginasVinyl Strip Flooringjuli_radAinda não há avaliações
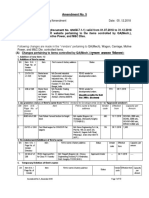
- Vendor Directory Amendment No - 5Documento10 páginasVendor Directory Amendment No - 5annayya.chandrashekar Civil EngineerAinda não há avaliações
- Water Chemistry - Mark Benjamin - 2nd EdDocumento935 páginasWater Chemistry - Mark Benjamin - 2nd EdPedro Casa Grande Rosa95% (19)
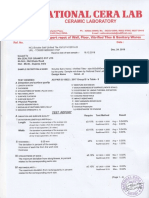
- 12 - National Cera Lab Test Report - 600x1200 MM - 24.12.2019Documento3 páginas12 - National Cera Lab Test Report - 600x1200 MM - 24.12.2019Shaikh MohammedHanifSultanAinda não há avaliações
- Flotation Mechanism Design For Improved Metallurgical and Energy PerformanceDocumento14 páginasFlotation Mechanism Design For Improved Metallurgical and Energy PerformanceCatalinaSoledadBelloCarrascoAinda não há avaliações
- 1 21 PDFDocumento21 páginas1 21 PDFray m deraniaAinda não há avaliações
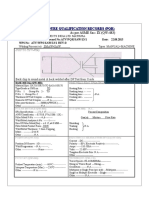
- Procedure Qualification Records (PQR)Documento2 páginasProcedure Qualification Records (PQR)amine algAinda não há avaliações
- Injection Wells - An Introduction To Their Use, Operation and RegulationDocumento16 páginasInjection Wells - An Introduction To Their Use, Operation and RegulationrakicbgAinda não há avaliações
- Biosuite Qd10 Ghs Sds - Us v04Documento6 páginasBiosuite Qd10 Ghs Sds - Us v04izzybjAinda não há avaliações
- JBC Common Boiler FormulasDocumento12 páginasJBC Common Boiler Formulasnesrine10Ainda não há avaliações
- Claytone Af TDS (En)Documento2 páginasClaytone Af TDS (En)محمد عزت100% (1)
- 1100-Data Sheets PDFDocumento3 páginas1100-Data Sheets PDFPaturu VijayAinda não há avaliações
- Cheetham Salt BrochureDocumento8 páginasCheetham Salt BrochureSamscribdingAinda não há avaliações
- MSDS Accelerator MBT 2-Mercaptobenzothiazole KemaiDocumento7 páginasMSDS Accelerator MBT 2-Mercaptobenzothiazole KemaicarlosAinda não há avaliações
- Types of Chemical ReactionsDocumento35 páginasTypes of Chemical ReactionsJemina R. B. EspedillonAinda não há avaliações
- Ethylene Decomposition Relief Sizing High Pressure Polyethylene IndustryDocumento11 páginasEthylene Decomposition Relief Sizing High Pressure Polyethylene Industryoscarxsmith01Ainda não há avaliações
- F.4 Acids and Exercise)Documento69 páginasF.4 Acids and Exercise)arielshy100% (5)
- Hanwha Total PP HJ700Documento2 páginasHanwha Total PP HJ700Nguyễn Hồng NamAinda não há avaliações
- Factors Affecting Rate of EvaporationDocumento12 páginasFactors Affecting Rate of EvaporationVikram DasAinda não há avaliações
- Fischer-Tropsch: IncorporationDocumento6 páginasFischer-Tropsch: Incorporationamirhosein saqafiAinda não há avaliações
- Grade 11 Physics Module6Documento83 páginasGrade 11 Physics Module6JohnRenzoMolinarAinda não há avaliações
- Model M05 Non-Metallic Design Level 2: Service & Operating ManualDocumento33 páginasModel M05 Non-Metallic Design Level 2: Service & Operating ManualTrungGVAinda não há avaliações
- Alb BiosDocumento2 páginasAlb BiosrichardAinda não há avaliações
- Essential Variables API 1104Documento4 páginasEssential Variables API 1104Madidj_2014Ainda não há avaliações
- EjemploDocumento128 páginasEjemploviryi09Ainda não há avaliações
- UL PresentationDocumento18 páginasUL Presentationsethhcohen11Ainda não há avaliações
- Lime Based MortarDocumento39 páginasLime Based MortarAparna Kumar100% (2)
- Chock FastDocumento25 páginasChock FastBrajko NikolaAinda não há avaliações
- Solder Re Flow Guide For Surface Mount DevicesDocumento13 páginasSolder Re Flow Guide For Surface Mount DevicesWandyy GonçalvesAinda não há avaliações