Você também pode gostar
- Acute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Documento11 páginasAcute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Roscheen Berg TutorAinda não há avaliações
- Acute GastroenteritisDocumento51 páginasAcute GastroenteritisuouoAinda não há avaliações
- Diarrhea - StatPearls - NCBI BookshelfDocumento4 páginasDiarrhea - StatPearls - NCBI BookshelfIndira SellyAinda não há avaliações
- Dehydration Isonatremic, Hyponatremic, andDocumento15 páginasDehydration Isonatremic, Hyponatremic, andalfredoibcAinda não há avaliações
- Case ManagementDocumento11 páginasCase ManagementGabrielle CatalanAinda não há avaliações
- Acute GastroenteritisDocumento11 páginasAcute GastroenteritisIneke PutriAinda não há avaliações
- Pediatrics in Review. Dehydration 2015Documento14 páginasPediatrics in Review. Dehydration 2015Jorge Eduardo Espinoza Rios100% (2)
- Management of Acute Gastroenteritis in Children: Pathophysiology in The UKDocumento6 páginasManagement of Acute Gastroenteritis in Children: Pathophysiology in The UKMarnia SulfianaAinda não há avaliações
- Management of Acute Diarrhea in Emergency RoomDocumento12 páginasManagement of Acute Diarrhea in Emergency RoomRajiv KabadAinda não há avaliações
- DeshidratacionDocumento14 páginasDeshidratacionAlvaro Andres Flores JimenezAinda não há avaliações
- Klasifikasi Diare Pada AnakDocumento15 páginasKlasifikasi Diare Pada AnakTia UtamiAinda não há avaliações
- Gastroenteritis:: Diarrhea & DehydrationDocumento26 páginasGastroenteritis:: Diarrhea & DehydrationcorsaruAinda não há avaliações
- Diarrhea CaseDocumento8 páginasDiarrhea CaseStarr NewmanAinda não há avaliações
- Ujian IhbDocumento17 páginasUjian IhbAnonymous obEaRZ6P85Ainda não há avaliações
- CholeraDocumento21 páginasCholeraMASII100% (1)
- Practice Essentials: Clinical PresentationDocumento3 páginasPractice Essentials: Clinical PresentationtesaAinda não há avaliações
- Diarrhea in ChildrenDocumento23 páginasDiarrhea in ChildrenSudeshna YadavAinda não há avaliações
- Diarrhea GuidelineDocumento29 páginasDiarrhea GuidelineMonica GabrielAinda não há avaliações
- Dan L Ellsbury, MD, FAAPDocumento8 páginasDan L Ellsbury, MD, FAAPfaruuukAinda não há avaliações
- Treatment of DiarrheaDocumento6 páginasTreatment of DiarrheaVictor TayoAinda não há avaliações
- Biochemical Aspect of DiarrheaDocumento17 páginasBiochemical Aspect of DiarrheaLiz Espinosa0% (1)
- Diarrhea: Practice Essentials, Background, PathophysiologyDocumento6 páginasDiarrhea: Practice Essentials, Background, PathophysiologyBilal El BariAinda não há avaliações
- Guidelines For Managing Acute Gastroenteritis Based On A Systematic Review of Published ResearchDocumento7 páginasGuidelines For Managing Acute Gastroenteritis Based On A Systematic Review of Published ResearchnikopkunairAinda não há avaliações
- Gastroenteritis: Presented by BSCN - Krchn. Paul Mutie Cyrus Pwani UniversityDocumento35 páginasGastroenteritis: Presented by BSCN - Krchn. Paul Mutie Cyrus Pwani UniversityAleeya rizviAinda não há avaliações
- Diarrhea Diarrhea: Signs and SymptomsDocumento10 páginasDiarrhea Diarrhea: Signs and SymptomsMelhor TrioAinda não há avaliações
- Epidemiology of CholeraDocumento26 páginasEpidemiology of CholeraSoodn Kang SoodnAinda não há avaliações
- Acute Diarrhea: By: Mohamad El-Shar, MDDocumento34 páginasAcute Diarrhea: By: Mohamad El-Shar, MDMohamad El SharAinda não há avaliações
- Gastroenteritis Gastrointestinal Tract: Clostridium DifficileDocumento14 páginasGastroenteritis Gastrointestinal Tract: Clostridium DifficilemichunmeeadAinda não há avaliações
- CholeraDocumento6 páginasCholeraSaumya ShrirupAinda não há avaliações
- BRS Pediatrics (Dragged)Documento3 páginasBRS Pediatrics (Dragged)amjdnuaimyAinda não há avaliações
- Gastro Inter It IsDocumento3 páginasGastro Inter It IsDhea Imas WijayantiAinda não há avaliações
- 21.child With Diarrhea and Vomiting-SeminarDocumento65 páginas21.child With Diarrhea and Vomiting-SeminarRhomizal MazaliAinda não há avaliações
- Clinical Review: Acute Gastroenteritis in ChildrenDocumento6 páginasClinical Review: Acute Gastroenteritis in ChildrenWildan Wisnu WardayaAinda não há avaliações
- Diarrea Crónica UPTODATEDocumento6 páginasDiarrea Crónica UPTODATEConsuelo RiveraAinda não há avaliações
- Diarrea CrónicaDocumento6 páginasDiarrea CrónicaConsuelo RiveraAinda não há avaliações
- GastroenteritisDocumento14 páginasGastroenteritisJils SureshAinda não há avaliações
- Acute Infectious Diarrhea: TOC GIDocumento14 páginasAcute Infectious Diarrhea: TOC GIFerry EffendiAinda não há avaliações
- Acute GastroenteritisDocumento48 páginasAcute GastroenteritisAbel QuisquisAinda não há avaliações
- Case Report GastroenteritisDocumento36 páginasCase Report GastroenteritisDaisy DuckAinda não há avaliações
- Diarrhea 1Documento5 páginasDiarrhea 1Mohammed Taha Al-nuaimyAinda não há avaliações
- DIARRHEADocumento44 páginasDIARRHEAKristin Masehathena BerutuAinda não há avaliações
- Gastroenteritis in ChildrenDocumento48 páginasGastroenteritis in ChildrenKelsingra FitzChivalry FarseerAinda não há avaliações
- Gastroenteritis in Adults and Older Children: EpidemiologyDocumento4 páginasGastroenteritis in Adults and Older Children: Epidemiologyjotq19Ainda não há avaliações
- Cholera: DR - Haifa Yagoub OsmanDocumento24 páginasCholera: DR - Haifa Yagoub OsmanAlex SamAinda não há avaliações
- Community Health Nursing-II DiarrheaDocumento4 páginasCommunity Health Nursing-II DiarrheaPriya bhattiAinda não há avaliações
- Chapter 45: Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDocumento14 páginasChapter 45: Nursing Care of A Family When A Child Has A Gastrointestinal DisorderAlyssaGrandeMontimor100% (3)
- Presentation 3Documento14 páginasPresentation 3olayemi morakinyoAinda não há avaliações
- Acute Gastroenteritis in ChildrenDocumento24 páginasAcute Gastroenteritis in ChildrenramwshAinda não há avaliações
- Diarrhoea in TravellersDocumento5 páginasDiarrhoea in TravellersMazo KhanAinda não há avaliações
- CholeraDocumento36 páginasCholeraPaulAinda não há avaliações
- Nursing Care of Children With Indian Childhood Cirrhosis, Wilsons Disesase, Reyes SyndromeDocumento26 páginasNursing Care of Children With Indian Childhood Cirrhosis, Wilsons Disesase, Reyes SyndromeDivya Nair100% (2)
- Acute GastroenteritisDocumento54 páginasAcute GastroenteritisVincent LaranjoAinda não há avaliações
- Fluidoterapia 3Documento16 páginasFluidoterapia 3Gera DAinda não há avaliações
- Junior Intern Review - Oral Revalida 2016Documento170 páginasJunior Intern Review - Oral Revalida 2016Cyrus ZalameaAinda não há avaliações
- ShigellosisDocumento14 páginasShigellosisMuhammad GetsoAinda não há avaliações
- Dehydration: Royal Medical Services Provider Unit Nursing Continuing Education and Training DepartmentDocumento34 páginasDehydration: Royal Medical Services Provider Unit Nursing Continuing Education and Training DepartmentJanuaryAinda não há avaliações
- Anterior Enteritis: Rodney L. BelgraveDocumento3 páginasAnterior Enteritis: Rodney L. BelgraveJennifer Vargas HerreraAinda não há avaliações
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisNo EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisNota: 3 de 5 estrelas3/5 (1)
- A Simple Guide to Celiac Disease and Malabsorption DiseasesNo EverandA Simple Guide to Celiac Disease and Malabsorption DiseasesAinda não há avaliações
- KimPhan PediatricDocumento4 páginasKimPhan PediatricStephen Leeper100% (2)
- Maintaining Fluid & Electrolyte Balance in The BodyDocumento124 páginasMaintaining Fluid & Electrolyte Balance in The BodyKingJayson Pacman06100% (1)
- Am J Clin Nutr 2016 Maughan 717 23Documento7 páginasAm J Clin Nutr 2016 Maughan 717 23sfvsvsAinda não há avaliações
- Acute Viral Gastroenteritis in Children in Resource-Rich Countries: Management and PreventionDocumento25 páginasAcute Viral Gastroenteritis in Children in Resource-Rich Countries: Management and Preventiondaniso12Ainda não há avaliações
- Hydration Research PosterDocumento1 páginaHydration Research Posterapi-310111771Ainda não há avaliações
- Gastroenteritis An Evidence Based Approach To Typical Vomiting, Diarrhea, and DehydrationDocumento20 páginasGastroenteritis An Evidence Based Approach To Typical Vomiting, Diarrhea, and DehydrationpancseszAinda não há avaliações
- Management of Childhood Diarrhea by Healthcare Professionals in Low Income CountriesDocumento40 páginasManagement of Childhood Diarrhea by Healthcare Professionals in Low Income CountriesrafaAinda não há avaliações
- Slemani Pediatric Teaching Hospital GuidelinesDocumento93 páginasSlemani Pediatric Teaching Hospital GuidelinesHeersh RaofAinda não há avaliações
- VAD Vesikari Scoring ManualDocumento51 páginasVAD Vesikari Scoring Manualmuhamad mukhtarAinda não há avaliações
- Acute Diarrhoeal DiseaseDocumento68 páginasAcute Diarrhoeal DiseasePratima Matli100% (1)
- Food PoisoningDocumento11 páginasFood PoisoningLeanne Teh100% (1)
- ORS Package InsertDocumento1 páginaORS Package InsertwhothehellisarcticmonkeysAinda não há avaliações
- September 16 - IMCIDocumento5 páginasSeptember 16 - IMCIJonas Marvin AnaqueAinda não há avaliações
- Unit-6 New Born IgnouDocumento26 páginasUnit-6 New Born IgnouVijay MgAinda não há avaliações
- Referat Arlha PemDocumento65 páginasReferat Arlha PemDicky Delonge LesmanaAinda não há avaliações
- Home Made ORSDocumento4 páginasHome Made ORSTrajan AureliusAinda não há avaliações
- Emetics and Antiemetics DrugsDocumento15 páginasEmetics and Antiemetics DrugsrajenderAinda não há avaliações
- Acute Gastroenteritis in Paediatrics 1Documento43 páginasAcute Gastroenteritis in Paediatrics 1Imran FaisalAinda não há avaliações
- ACSM Position Stand - Exercise and Fluid Replacement - Medicine & Science in Sports & ExerciseDocumento7 páginasACSM Position Stand - Exercise and Fluid Replacement - Medicine & Science in Sports & ExerciseDiógenes OliveiraAinda não há avaliações
- By Mayo Clinic Staff: DiarrheaDocumento6 páginasBy Mayo Clinic Staff: DiarrheaJamelyn GongoraAinda não há avaliações
- Who Dehidrasi PG 17 PDFDocumento52 páginasWho Dehidrasi PG 17 PDFSasha ManoAinda não há avaliações
- Diare Dan DehidrasiDocumento61 páginasDiare Dan DehidrasiOktavian Rizki IlahiAinda não há avaliações
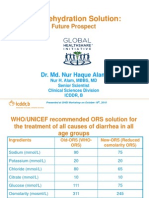
- Oral Rehydration Solution:: Future ProspectDocumento48 páginasOral Rehydration Solution:: Future ProspectmustikaarumAinda não há avaliações
- Cholera: by Jack Eilers and Lucas LagerlingDocumento12 páginasCholera: by Jack Eilers and Lucas Lagerlingapi-208350315Ainda não há avaliações
- Pediatrics-in-Review 1989 - Acute Diarrhea in Children PDFDocumento10 páginasPediatrics-in-Review 1989 - Acute Diarrhea in Children PDFmob3Ainda não há avaliações
- Cholera Case ManagementDocumento35 páginasCholera Case ManagementRegnold MAinda não há avaliações
- Hygiene Promotion Training For Community Mobilisers - Course OutlineDocumento60 páginasHygiene Promotion Training For Community Mobilisers - Course OutlineLaura Tomasa83% (6)
- Paediatric Emergencies2Documento244 páginasPaediatric Emergencies2Amber MonroeAinda não há avaliações
- Pediatric Gastroenterology AlgorithmeDocumento118 páginasPediatric Gastroenterology AlgorithmeBenazier Marcella Besmaya100% (2)
- Food PoisoningDocumento24 páginasFood PoisoningSena AjahAinda não há avaliações