Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- On MCH and Maternal Health in BangladeshDocumento46 páginasOn MCH and Maternal Health in BangladeshTanni ChowdhuryAinda não há avaliações
- Cwu Ong TwinDocumento14 páginasCwu Ong TwinAiman ArifinAinda não há avaliações
- Iloilo City Regulation Ordinance 2015-163Documento5 páginasIloilo City Regulation Ordinance 2015-163Iloilo City CouncilAinda não há avaliações
- Obstetrics & Gynaecology 2019-2008 Regular-Supplementary Group Wise Question Papers WBUHS PDFDocumento14 páginasObstetrics & Gynaecology 2019-2008 Regular-Supplementary Group Wise Question Papers WBUHS PDFAditya BarmanAinda não há avaliações
- History-Taking & Physical Examination by DR Samer Abu EidehDocumento48 páginasHistory-Taking & Physical Examination by DR Samer Abu EidehAbdullah MatarAinda não há avaliações
- Konsep Askeb KomunitasDocumento58 páginasKonsep Askeb Komunitassulthoni ikaAinda não há avaliações
- Placenta Previa, Accreta, & Vasa Previa 2006Documento15 páginasPlacenta Previa, Accreta, & Vasa Previa 2006Ika Agustin0% (1)
- 3rd Stage of Labour PDFDocumento15 páginas3rd Stage of Labour PDFvarshasharma05Ainda não há avaliações
- Prenatal and Postnatal CareDocumento5 páginasPrenatal and Postnatal Caresarguss14100% (7)
- DR Amit Gupta - Medical Institute For Screening TestDocumento122 páginasDR Amit Gupta - Medical Institute For Screening TestEducation PlazaAinda não há avaliações
- Kehamilan Persalinan NifasDocumento29 páginasKehamilan Persalinan NifaschoiimmaAinda não há avaliações
- Hyperglycemia in PregnancyDocumento17 páginasHyperglycemia in PregnancyIza WidzAinda não há avaliações
- Skilled Birth Attendant (SBA) and Home Delivery in India: A Geographical StudyDocumento8 páginasSkilled Birth Attendant (SBA) and Home Delivery in India: A Geographical StudyInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- CE Doula Brochure August 1 2022Documento1 páginaCE Doula Brochure August 1 2022Raquel Orozco VargasAinda não há avaliações
- English For Midwife ConversationDocumento3 páginasEnglish For Midwife Conversationgilang rajasaAinda não há avaliações
- 137-Article Text-304-1-10-20200309Documento7 páginas137-Article Text-304-1-10-20200309agustina silalahiAinda não há avaliações
- Malpresentation: &malpositionDocumento16 páginasMalpresentation: &malpositionRamadan MusseAinda não há avaliações
- TS Circ025-2015Documento11 páginasTS Circ025-2015zaldusalvaradoAinda não há avaliações
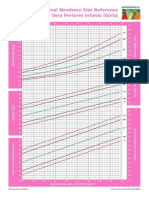
- Intergrowth21 Newborn Size Reference Charts (Girls)Documento2 páginasIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyAinda não há avaliações
- Placenta Previa: Introduction and DeffinitionDocumento4 páginasPlacenta Previa: Introduction and DeffinitionPriyaAinda não há avaliações
- AbortionDocumento11 páginasAbortionKopal GargAinda não há avaliações
- Complications of Twin Pregnancy: by Harsh SharmaDocumento19 páginasComplications of Twin Pregnancy: by Harsh SharmakushalAinda não há avaliações
- 1.mal PresentationDocumento75 páginas1.mal PresentationhabtamuAinda não há avaliações
- Persalinan. Yogyakarta: Yayasan Essentia MedicaDocumento2 páginasPersalinan. Yogyakarta: Yayasan Essentia MedicaYemimaAinda não há avaliações
- How To Diagnose PROM & PPROM - Cahara AdhiDocumento20 páginasHow To Diagnose PROM & PPROM - Cahara AdhiAmarendra Wardhana100% (1)
- Antepartum HemorrhageDocumento52 páginasAntepartum HemorrhageKomalah ChenasammyAinda não há avaliações
- Jordie-Prenatal Care StudygramDocumento7 páginasJordie-Prenatal Care StudygramNoreen Hannah GabrielAinda não há avaliações
- Exercise Prescription in Pre and Post-NatalDocumento63 páginasExercise Prescription in Pre and Post-NatalSim ShkAinda não há avaliações
- Abortion Is The Termination of A Pregnancy AfterDocumento6 páginasAbortion Is The Termination of A Pregnancy AfterTitia Pawifi ThaitangAinda não há avaliações
- Robson Classification - Implementation ManualDocumento56 páginasRobson Classification - Implementation ManualJuan Miguel PangilinanAinda não há avaliações