Você também pode gostar
- Control Aspects of Prosthetics and Orthotics: Proceedings of the IFAC Symposium, Ohio, USA, 7-9 May 1982No EverandControl Aspects of Prosthetics and Orthotics: Proceedings of the IFAC Symposium, Ohio, USA, 7-9 May 1982Ainda não há avaliações
- Limb Reconstruction SystemDocumento83 páginasLimb Reconstruction SystemGermán0% (1)
- PFC Sigma KneeDocumento36 páginasPFC Sigma KneeKaustubh KeskarAinda não há avaliações
- American Academy of Orthotists & ProsthetistsDocumento14 páginasAmerican Academy of Orthotists & ProsthetistsAndres UlloaAinda não há avaliações
- 501k StrykerDocumento12 páginas501k StrykerFrancisco100% (1)
- New Guidance On Product Family Adoption For Radiation Sterilization: AAMI TIR 35:2016Documento39 páginasNew Guidance On Product Family Adoption For Radiation Sterilization: AAMI TIR 35:2016RakeshAinda não há avaliações
- Double GlovingDocumento24 páginasDouble GlovingCarlos Rios100% (1)
- Amvex Intermittent Vacuum Regulator Manual PDFDocumento4 páginasAmvex Intermittent Vacuum Regulator Manual PDFPeter ayalaAinda não há avaliações
- Study Materials On Needles PDFDocumento24 páginasStudy Materials On Needles PDFzilangamba_s4535Ainda não há avaliações
- Zimmer ML Taper Hip Prosthesis Surgical TechniqueDocumento18 páginasZimmer ML Taper Hip Prosthesis Surgical TechniqueIchigo SnijdersAinda não há avaliações
- Hierarchical Task Analysis: Developments, Applications, and ExtensionsDocumento25 páginasHierarchical Task Analysis: Developments, Applications, and ExtensionsAndrea CamposAinda não há avaliações
- AllofitST Surgical TechDocumento16 páginasAllofitST Surgical TechAlexandru DumitrescuAinda não há avaliações
- Laminectomy Set MJK 1Documento10 páginasLaminectomy Set MJK 1Yusuf HermawanAinda não há avaliações
- Implant Stability - Measuring DevicesDocumento19 páginasImplant Stability - Measuring DevicesÁgnes Kocsis100% (1)
- 19-Microendoscopic Lumbar DiscectomyDocumento8 páginas19-Microendoscopic Lumbar DiscectomyNewton IssacAinda não há avaliações
- ATTUNE S+ Master Content Deck DSUS - JRC - 0517 - 2142Documento82 páginasATTUNE S+ Master Content Deck DSUS - JRC - 0517 - 2142medtechy100% (1)
- Day 2 - Friday - 0830 AM - Nick PetrickDocumento57 páginasDay 2 - Friday - 0830 AM - Nick PetrickPrevent Cancer FoundationAinda não há avaliações
- Versys Fiber Metal Taper Hip Prosthesis Surgical TechniqueDocumento16 páginasVersys Fiber Metal Taper Hip Prosthesis Surgical TechniqueSaumil ShahAinda não há avaliações
- Tradeoffs Amongst Fatigue Wear and Oxidation Resistance of Cross-Linked Ultra-High Molecular Weight PolyethyleneDocumento13 páginasTradeoffs Amongst Fatigue Wear and Oxidation Resistance of Cross-Linked Ultra-High Molecular Weight PolyethyleneNeuza PimentaAinda não há avaliações
- Design of A Prosthesis For Running in Composite MaterialsDocumento12 páginasDesign of A Prosthesis For Running in Composite MaterialsginkenoAinda não há avaliações
- Introduction To LOINC/RSNA PlaybookDocumento35 páginasIntroduction To LOINC/RSNA PlaybookDaniel Vreeman100% (1)
- Global Top 100 Manufacturers of Orthopedic & Prosthetic Devices: A Thorough Analysis of The Technologies and TrendsDocumento4 páginasGlobal Top 100 Manufacturers of Orthopedic & Prosthetic Devices: A Thorough Analysis of The Technologies and Trendsriya jain0% (1)
- Corail Surgical Technique Revision 1 PDFDocumento20 páginasCorail Surgical Technique Revision 1 PDFKaustubh KeskarAinda não há avaliações
- Is 13726 2002Documento19 páginasIs 13726 2002john23141Ainda não há avaliações
- Secur-Fit Advanced: Surgical TechniqueDocumento28 páginasSecur-Fit Advanced: Surgical TechniqueX ComAinda não há avaliações
- ASFNR Guidelines For DTIDocumento5 páginasASFNR Guidelines For DTIangel_of_heavenAinda não há avaliações
- Shoulder Arthroplasty WIC - Dr. LSDocumento56 páginasShoulder Arthroplasty WIC - Dr. LSDifitasari Cipta Perdana100% (1)
- Managing Sciatica and Radicular Pain in Primary Care PracticeDocumento153 páginasManaging Sciatica and Radicular Pain in Primary Care PracticeElena MadalinaAinda não há avaliações
- Amvex Continuous Vacuum Regulator ManualDocumento4 páginasAmvex Continuous Vacuum Regulator ManualPeter AyalaAinda não há avaliações
- k162919 Device DescriptionDocumento7 páginask162919 Device DescriptionjsdanielinAinda não há avaliações
- Rotational Flap Closure of 1st and 5nth Met HeadDocumento8 páginasRotational Flap Closure of 1st and 5nth Met HeadleahbayAinda não há avaliações
- Synergy CementlessDocumento32 páginasSynergy CementlessSergiu Plesca100% (1)
- TR300 Benign Hysterectomy TR300.GYN: Da Vinci Si™/ Xi™ SystemDocumento3 páginasTR300 Benign Hysterectomy TR300.GYN: Da Vinci Si™/ Xi™ SystemShayne JacobsonAinda não há avaliações
- Target Electric Blanket InstructionsDocumento15 páginasTarget Electric Blanket Instructionsbritt16110% (1)
- Thoracic Endoscopic Spine Surgery A ComprehensiveDocumento11 páginasThoracic Endoscopic Spine Surgery A Comprehensivesanjay chhawraAinda não há avaliações
- Mhdpow PDFDocumento95 páginasMhdpow PDFGana PathiAinda não há avaliações
- FDA Biocompatibility PDFDocumento7 páginasFDA Biocompatibility PDFFelipe ValleAinda não há avaliações
- Review - Presby Residency ManualDocumento400 páginasReview - Presby Residency ManualSneha SutharAinda não há avaliações
- Set Torakotomi + Sternotomi (Basic) DR ArmanDocumento6 páginasSet Torakotomi + Sternotomi (Basic) DR ArmanDonny JatmikoAinda não há avaliações
- Amputee Course 2009Documento6 páginasAmputee Course 2009ptannenbaumAinda não há avaliações
- 693 Standard C-Cem Impl. Instr. OP en 2012-04-001lDocumento24 páginas693 Standard C-Cem Impl. Instr. OP en 2012-04-001lYerika Cañizalez de PartidasAinda não há avaliações
- Microneuro Surgery SetDocumento3 páginasMicroneuro Surgery SetYeni SetiowatiAinda não há avaliações
- Trochanteric Nail 170 & 180: Gamma3Documento44 páginasTrochanteric Nail 170 & 180: Gamma3alexAinda não há avaliações
- Classification of Medical ProceduresDocumento1.401 páginasClassification of Medical Proceduresthe_albenaAinda não há avaliações
- York, PA 17402 USA: 510 (K) SummaryDocumento6 páginasYork, PA 17402 USA: 510 (K) SummaryASHOKAinda não há avaliações
- c40402 Sterile ContainerAESCULAPDocumento108 páginasc40402 Sterile ContainerAESCULAPIfan RizkyAinda não há avaliações
- IQ4I Research & Consultancy Published A New Report On "Catheters Global Market - Forecast To 2022"Documento4 páginasIQ4I Research & Consultancy Published A New Report On "Catheters Global Market - Forecast To 2022"VinayAinda não há avaliações
- Large Medium ExternalfixatorsDocumento42 páginasLarge Medium ExternalfixatorsZulfadli Salleh0% (1)
- Ao Foundation - Handouts - English - Principles of Fracture Fixation - Handout - v2Documento12 páginasAo Foundation - Handouts - English - Principles of Fracture Fixation - Handout - v2raz2000Ainda não há avaliações
- SJAMS 43B 750 754 Thesis Tibial PlateauDocumento5 páginasSJAMS 43B 750 754 Thesis Tibial PlateauNisheshJainAinda não há avaliações
- Final Qa TablesDocumento15 páginasFinal Qa Tablesapi-385172083Ainda não há avaliações
- 2020 Book Biomaterials-AndMicrofluidicsDocumento176 páginas2020 Book Biomaterials-AndMicrofluidicsAlejandra CastillaAinda não há avaliações
- James v. Bono, Richard D. Scott (Eds.) - Revision Total Knee Arthroplasty (2018, Springer) (10.1007 - 978!3!319-67344-8) - Libgen - LiDocumento421 páginasJames v. Bono, Richard D. Scott (Eds.) - Revision Total Knee Arthroplasty (2018, Springer) (10.1007 - 978!3!319-67344-8) - Libgen - Lisergio montesAinda não há avaliações
- Umbilicalherniarepair: Overview of Approaches and Review of LiteratureDocumento16 páginasUmbilicalherniarepair: Overview of Approaches and Review of LiteratureVictor Matias BarriosAinda não há avaliações
- NoThing Left Behind Policy v5 PDFDocumento54 páginasNoThing Left Behind Policy v5 PDFO.r. Cadz100% (1)
- Miles Operation - Abdominoperineal Excision - Rectal CADocumento5 páginasMiles Operation - Abdominoperineal Excision - Rectal CASpencer DempseyAinda não há avaliações
- Understanding MRI: Basic MR Physics For PhysiciansDocumento15 páginasUnderstanding MRI: Basic MR Physics For PhysiciansErick Roa GandicaAinda não há avaliações
- Exeter V40: Femoral Stem Using Exeter BroachDocumento20 páginasExeter V40: Femoral Stem Using Exeter BroachzakAinda não há avaliações
- Lifestyle PDFDocumento19 páginasLifestyle PDFManish RajAinda não há avaliações
- AdhikamasaDocumento12 páginasAdhikamasaushasrivathsanAinda não há avaliações
- v1 Ri - Knee Navigation Technical Presentation 0621 1Documento331 páginasv1 Ri - Knee Navigation Technical Presentation 0621 1Sagaram ShashidarAinda não há avaliações
- DownloadDocumento4 páginasDownloadSagaram ShashidarAinda não há avaliações
- Form - VI (Knee Component) Price DetailsDocumento24 páginasForm - VI (Knee Component) Price DetailsSagaram ShashidarAinda não há avaliações
- Gopichandana Mudradharana VidhiDocumento6 páginasGopichandana Mudradharana VidhiSagaram ShashidarAinda não há avaliações
- Patella Instability PDFDocumento14 páginasPatella Instability PDFSagaram ShashidarAinda não há avaliações
- Acknowledge Receipt RequestDocumento1 páginaAcknowledge Receipt RequestSagaram ShashidarAinda não há avaliações
- Data Management Rescues WhitepaperDocumento2 páginasData Management Rescues WhitepaperSagaram ShashidarAinda não há avaliações
- Trikal SandhyaDocumento22 páginasTrikal Sandhyamak350Ainda não há avaliações
- Case Report FormDocumento1 páginaCase Report FormSagaram ShashidarAinda não há avaliações
- Anatomy and Biomechanics of The KneeDocumento4 páginasAnatomy and Biomechanics of The KneeSagaram ShashidarAinda não há avaliações
- Chap 55Documento157 páginasChap 55Sagaram ShashidarAinda não há avaliações
- The Paper Trail: CRFS, Source Documents and Data Collection ToolsDocumento5 páginasThe Paper Trail: CRFS, Source Documents and Data Collection ToolsSagaram ShashidarAinda não há avaliações
- Application Form Recombinant DnaDocumento8 páginasApplication Form Recombinant DnaSagaram ShashidarAinda não há avaliações
- Freedom Knee Surgical Technique PrintDocumento16 páginasFreedom Knee Surgical Technique PrintSagaram ShashidarAinda não há avaliações
- A Method For Cleaning Clinical Trial DatasetsDocumento9 páginasA Method For Cleaning Clinical Trial DatasetsSagaram ShashidarAinda não há avaliações
- The Paper Trail: CRFS, Source Documents and Data Collection ToolsDocumento5 páginasThe Paper Trail: CRFS, Source Documents and Data Collection ToolsSagaram ShashidarAinda não há avaliações
- 16 Quality of Spon ReportingDocumento5 páginas16 Quality of Spon ReportingSagaram ShashidarAinda não há avaliações
- Status of Spontaneous Reporting of Adverse Drug Reaction by Physicians in DelhiDocumento8 páginasStatus of Spontaneous Reporting of Adverse Drug Reaction by Physicians in DelhiSagaram ShashidarAinda não há avaliações
- Access Patient InfoDocumento36 páginasAccess Patient InfoSagaram ShashidarAinda não há avaliações
- Lecture 5Documento50 páginasLecture 5Sagaram ShashidarAinda não há avaliações
- Sagaram Sharath KumarDocumento1 páginaSagaram Sharath KumarSagaram ShashidarAinda não há avaliações
- Vaikhanasa AgamaDocumento259 páginasVaikhanasa AgamaSagaram Shashidar88% (8)
- To Convert First Name and Last Name in Proper CaseDocumento1 páginaTo Convert First Name and Last Name in Proper CaseSagaram ShashidarAinda não há avaliações
- InTech-Management of Bone Loss in Primary and Revision Knee Replacement SurgeryDocumento25 páginasInTech-Management of Bone Loss in Primary and Revision Knee Replacement SurgerySagaram ShashidarAinda não há avaliações
- New Microsoft Word DocumentDocumento31 páginasNew Microsoft Word DocumentSagaram ShashidarAinda não há avaliações
- Lctr4.3 KJS UPNISHADSDocumento17 páginasLctr4.3 KJS UPNISHADSSagaram ShashidarAinda não há avaliações
- SC Perthub Single Cell OmicsDocumento34 páginasSC Perthub Single Cell OmicsGANYA U 2022 Batch,PES UniversityAinda não há avaliações
- Pioneer Car Stereo System DVH-735AVDocumento85 páginasPioneer Car Stereo System DVH-735AVJs LópezAinda não há avaliações
- Rotary Valve Functions BookletDocumento17 páginasRotary Valve Functions Bookletamahmoud3Ainda não há avaliações
- TMT Boron CoatingDocumento6 páginasTMT Boron Coatingcvolkan1100% (2)
- Slip Rings: SRI085 V100 - XX - XX - Xxx1XxDocumento3 páginasSlip Rings: SRI085 V100 - XX - XX - Xxx1XxMatheus Henrique MattiaAinda não há avaliações
- FI Printing Guide Vinyl-303Documento1 páginaFI Printing Guide Vinyl-303tomasykAinda não há avaliações
- T0000598REFTRGiDX 33RevG01052017 PDFDocumento286 páginasT0000598REFTRGiDX 33RevG01052017 PDFThanhAinda não há avaliações
- 3x Exemplar 2017 en PDFDocumento4 páginas3x Exemplar 2017 en PDFgudzalovAinda não há avaliações
- Database Programming With SQL 12-3: DEFAULT Values, MERGE, and Multi-Table Inserts Practice ActivitiesDocumento2 páginasDatabase Programming With SQL 12-3: DEFAULT Values, MERGE, and Multi-Table Inserts Practice ActivitiesFlorin CatalinAinda não há avaliações
- 1.summative-Test Math7Documento1 página1.summative-Test Math7Jaylor GaridoAinda não há avaliações
- API2000 Tank Venting CalcsDocumento5 páginasAPI2000 Tank Venting Calcsruhul01Ainda não há avaliações
- Workshop 2 Electrical Installations Single PhaseDocumento3 páginasWorkshop 2 Electrical Installations Single PhaseDIAN NUR AIN BINTI ABD RAHIM A20MJ0019Ainda não há avaliações
- Faculty: Geology Exploration Specialty: Geology Engineering Group: 123.6 Student: Asef Sadiqov Teacher: Afet Israfilova Theme: The EarthDocumento16 páginasFaculty: Geology Exploration Specialty: Geology Engineering Group: 123.6 Student: Asef Sadiqov Teacher: Afet Israfilova Theme: The EarthKenan RehmanAinda não há avaliações
- Translating Trig Graphs PDFDocumento4 páginasTranslating Trig Graphs PDFMark Abion ValladolidAinda não há avaliações
- Sqluser v11r1Documento199 páginasSqluser v11r1samnolenAinda não há avaliações
- TOEC8431120DDocumento522 páginasTOEC8431120Dvuitinhnhd9817Ainda não há avaliações
- SPE-183743-MS Maintaining Injectivity of Disposal Wells: From Water Quality To Formation PermeabilityDocumento19 páginasSPE-183743-MS Maintaining Injectivity of Disposal Wells: From Water Quality To Formation PermeabilityAminAinda não há avaliações
- Z Series: VZ-80 Series Portable Radio - VHF/UHFDocumento2 páginasZ Series: VZ-80 Series Portable Radio - VHF/UHFPrima SonyAinda não há avaliações
- Nomad Pro Operator ManualDocumento36 páginasNomad Pro Operator Manualdavid_stephens_29Ainda não há avaliações
- KD-131 Asme Viii Div3Documento2 páginasKD-131 Asme Viii Div3comar85Ainda não há avaliações
- 307-01 Automatic Transmission 10 Speed - Description and Operation - DescriptionDocumento12 páginas307-01 Automatic Transmission 10 Speed - Description and Operation - DescriptionCARLOS LIMADAAinda não há avaliações
- Chapter 3Documento23 páginasChapter 3pganoelAinda não há avaliações
- GS (2006) Vol 2 Rev20 S15 Steel ReinforcementDocumento14 páginasGS (2006) Vol 2 Rev20 S15 Steel ReinforcementLap Chun TUNGAinda não há avaliações
- Unit 07 Self-Test Chemistry Self TestDocumento2 páginasUnit 07 Self-Test Chemistry Self TestOluwatusin Ayo OluwatobiAinda não há avaliações
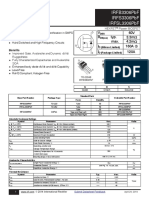
- Irfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADocumento12 páginasIrfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADirson Volmir WilligAinda não há avaliações
- A Tutorial On Spectral Sound Processing Using Max/MSP and JitterDocumento16 páginasA Tutorial On Spectral Sound Processing Using Max/MSP and Jittertramazio0% (1)
- Fiberglass Fire Endurance Testing - 1992Documento58 páginasFiberglass Fire Endurance Testing - 1992shafeeqm3086Ainda não há avaliações
- 2023-1509 TopSolid'Design Library Designer's GuideDocumento21 páginas2023-1509 TopSolid'Design Library Designer's GuideMáy TiệnAinda não há avaliações
- SM700 E WebDocumento4 páginasSM700 E WebrobertwebberAinda não há avaliações
- V. Activities: A. Directions: Do The Activity Below. (20 PTS.) Note: Work On This OfflineDocumento7 páginasV. Activities: A. Directions: Do The Activity Below. (20 PTS.) Note: Work On This OfflineKeith Neomi CruzAinda não há avaliações