Fort Campbell Daily Information Update
SUMMARY: 1) 2) 3) FREE Adventure Camp Oct. 6-9! (2x attached) Case Lot Sale at Commissary (attached) National Disabilities Month
1) FREE Adventure Camp Oct. 6-9! (2x attached) Thank you for your continued support for the Military-Extension Adventure Camps (MEAC)! We have our next camp in just 3 weeks and need your help to get more families signed up! We still have space for 16 people. If you wouldn't mind, please distributed the following email and/or attached flyer to all of the military families that you know. Thank you! Lauren Smith
2) Case Lot Sale at Commissary (attached) Attached is the list of items that will be available at this weekends' Case Lot Sale at the Fort Campbell Commissary. The sale beings today, 15 Sept, and runs through Sunday, 18 Sept. The case lot sale is great opportunity for savings, but please remind everyone that they should expect long lines!
3) National Disabilities Month Hello Everyone, Just a reminder about our upcoming event for October. In the past we have displayed art work submitted by the Special Education Classes from schools in our area at our National Disabilities luncheon in October; however, this year we thought we would try something different. We would like to invite parents, teachers or care givers to contribute stories about your child with special needs. Has your child achieved some major milestones in his/her life? What are the contributions your child has made to your Family? Every child is special, what makes your child so special to you? You can e-mail your articles to our office; you can drop them off to us; or you can mail them to us. We plan to make story boards and display them at our luncheon that will be held 27 October at Cole Park Commons. Tickets should go on sale in late September.
15 September 2011
Information Provided by FTCKY FRSA Network
Page 1 of 2
Fort Campbell Daily Information Update
If you have questions, feel free to call us any time. 270-798-2727 or my phone is 270-956-2529. Ann Brown ACS, EFMP Our main office phone is
15 September 2011
Information Provided by FTCKY FRSA Network
Page 2 of 2
Military-Extension Adventure Camp Backpacking 101 & Green River Paddle
Looking for an exciting family vacation? Join us on this FREE canoeing and backpacking adventure! October 6-9, 2011
NO GEAR? NO EXPERIENCE?
NO PROBLEM!
Join us for a multi-day canoe and backpacking experience on the Green River near Mammoth Cave, KY. FREE for service member parents and their children ages 14 -18! Families welcome from any state or branch of the military! Have a great time, reconnect, and spend quality time together while meeting other military families!!
To sign up or for more information, Please contact:
Lauren Smith Military Extension Adventure Camp Coordinator University of Kentucky (859) 257-3072 Lauren.w.smith@uky.edu Learn more at: http://www.ca.uky.edu/hes/fcs/militarycamp
Application Packet: 2011 Military-Extension Adventure Camps
The University of Kentucky Family and Consumer Sciences Extension is offering camps for military parents and their teenage children ages 14-18 to attend together! We have SEVEN different camps to choose from in 2011! Everything at the camps, including all meals, is FREE! The camps are open to military parents and their teenage children ages 14-18 from any state and from any branch of the military. This includes Active Duty, Reserve, and National Guard families. Priority will go to military parents/children who have experienced at least one deployment and who are geographically dispersed. These camps will be held:
June 20-24, 2011: White Water Rafting, Oakhill, West Virginia, Near Eastern KY Space for up to 28 participants (14 Service Members and 14 teenage children) June 30-July 3, 2011: Canoeing/Coastal Camping, Land between the Lakes, West KY Space for up to 20 participants (10 Service Members and 10 teenage children July 21-24, 2011: Backpacking 101 and Green River Paddle Trip, Mammoth Cave National Park, Southwest KY; Space for up to 20 participants (10 Service Members and 10 teenage children) July 29-31, 2011: The Red River Gorge Backpacking and Canoeing Experience Daniel Boone National Forest, Southeast KY; Space for up to 18 participants (9 Service Members and 9 teenage children) August 12-14, 2011: Wilderness Survival, Big Bone Lick, State Park, Northern KY Space for up to 20 participants (10 Service Members and 10 teenage children) September 16-18, 2011: Challenge Course/Corn Maze, Life Adventure Center, Central KY; Space for up to 50 participants (25 Service Members and 25 teenage children) December 2-4, 2011: Cold Weather Camping, Lake Cumberland, Southern KY Space for up to 20 participants (10 Service Members and 10 teenage children)
Parent/child teams can attend any of the seven camps. All you have to do is fill out the correct pages (see instructions) and return them to the address below by the deadline for the camp for which you are registering. Make sure you fill out the correct pages for the camp you choose to attend. Pages 2, 3, and 4 are to be filled out just once for the whole family. Every page from that point forward will need to be filled once for each participating individual. Print off extra copies of pages that correspond with the camp you wish to attend, and attach to original family packet. We will also need a copy of every persons insurance card. If accepted you will receive a packet in the mail two weeks before the camp your family is attending with all the information you need for that camp. If you have any questions, contact Lauren Smith, MilitaryExtension Adventure Camp Coordinator, at 859-257-3072 or lauren.w.smith@uky.edu. Return registration forms to: Lauren Smith Military-Extension Adventure Camp Project Coordinator University of Kentucky 115 Huguelet Drive Room 245 Scovell Hall Lexington, KY 40546 0064
Military-Extension Adventure Camp Registration Form
Please complete ALL information on pages 2-12 for ALL camps. PLEASE PRINT CLEARLY. PLEASE CHOOSE THE CAMP YOU WISH TO ATTEND*: *If you mark more than one, please indicate first choice, second choice, etc. _____ June 20-24, 2011: White Water Rafting (Application due by May 1, 2011) _____ June 30-July 3, 2011: Canoeing/Coastal Camping (Application due by May 31, 2011) _____ July 21-24, 2011: Backpacking 101 and Green River Paddle Trip (Application due by June 10, 2011) July 29-31: Red River Gorge Backpacking and Canoeing Experience (Application due by June 10, 2011) _____ August 12-14, 2011: Wilderness Survival (Application due by June 30, 2011) _____ September 16-18, 2011: Challenge Course/Corn Maze (Application due by June 30, 2011) _____ December 2-4, 2011: Cold Weather Camping (Application due by June 30, 2011) Todays Date: _________________ Primary Contact Name: ____________________________________ Service Member Parent/Guardian: __________________________________ Gender: ______ Age: _____ Teenage child #1: _______________________________________________ Gender: ______ Age: _____ Teenage child #2: _______________________________________________ Gender: ______ Age: _____ (Please add additional family members on back if more space is needed)
Address: ______________________________________________________________________ City: ________________________________________ State: _______ Zip: ________
Home Phone: _______________________ Cell Phone: ________________________________ E-mail for primary contact: ____________________________________________
Emergency Contact Name (other than someone attending): _____________________________ Work Phone: _____________________________ Cell Phone: ____________________________ Home Phone: _____________________________ Email: _______________________________ Deployment Status of Service Member in Family (check one): _____ Never deployed & no plans to deploy _____ Have been deployed once _____ Have been deployed more than once
Military-Extension Adventure Camp Registration Form
Branch of Service: _____ Air Force _____ Marines _____ Army _____ Navy _____ Coast Guard
Please Circle ONLY One:
Active Duty
Reserve
National Guard
How did you hear about Kentuckys Military-Extension Adventure camps? _____ Unit Family Readiness Group _____ Email list ____ ISFAC _____ Operation: Military Kids State Team member or website _____ Unit Newsletter _____ Other please list: _______________________________________
Any special accommodations needed for a family member? If so, please list:
Any special dietary needs for a family member? If so, please list:
Please return to:
Lauren Smith Military-Extension Adventure Camp Project Coordinator University of Kentucky 115 Huguelet Drive 245 Scovell Hall Lexington, KY 40546-0064 lauren.w.smith@uky.edu 859-257-3072
Note: Priority for slots at each camp will be done by date registration is received. If a camp is full, you will be given the option of being put on a waitlist for that camp or attending a different camp that is still open. If your family has been selected for one of the slots you will be contacted. You will then receive a participant packet at least two weeks prior to that camp that will include: general instructions, camp rules & guidelines, a packing list, directions, a tentative agenda, and emergency numbers. Once all slots are filled, any registrants who are not initially selected will be placed on a wait list and you will be notified accordingly.
Military-Extension Adventure Camp Registration Form
Military-Extension Adventure CAMP RULES & REGULATIONS
Absolutely no alcoholic beverages, drugs, explosives or firearms are allowed on camp premises. No smoking allowed in any building, smoking is allowed only in marked areas. Instructions will be included in your Participant Packet. Comfortable shoes should be worn at all times. Parking is permitted only in marked areas. Driving and parking instructions will be included in your Participant Packet. No pets are permitted at camp facilities. Service animals are allowed. A life jacket MUST be worn at all times by anyone around any waterfront area and during all water activities. This is a time to spend connect with your family. Cell phones should be used in emergencies only. In the event of an injury to anyone in your family, notify camp staff immediately. An incident report form must be completed for any injury that occurs. Please notify Kerri Ashurst of any medical or health problems of family members BEFORE you come to camp. She will inform medical and camp staff. It is the responsibility of the parent or guardian to make sure participating teenage children understand and know all the rules BEFORE attending camp. It is the responsibility of the parent or guardian to supervise their children at camp at all times. There is a zero tolerance policy at camp for bullying, fighting, physical or verbal abuse, sexual harassment, inappropriate touching, or corporal punishment of children. Anyone violating this rule will be asked to leave the camp premises immediately. Families are responsible for the cleanliness of the camp facilities. It should be as clean when you leave as it was when you arrived. We understand that if we do not meet these expectations, we may be dismissed from camp and will be responsible for transportation off the premises. Service Member Parent/Guardian: __________________________________ Teenage child #1: _______________________________________________ Teenage child #2: _______________________________________________ (add additional teenage children if more space is needed)
Military-Extension Adventure Camp Registration Form
Registration/Health Form and Insurance Form
The following information must be filled out for EACH family member that will be attending a Military-Extension Adventure camp. The information on this form is not part of the camper or staff acceptance process, but is gathered to assist us in identifying appropriate care. Health history must be filled out by parent/guardians of all minors (under age 18).
Name ____________________________________________________________________ Age _______________________ LAST FIRST MIDDLE
Home address _________________________________________________________________________________________ STREET ADDRESS STATE ZIP CITY
Phone __________________________________ Race*____________________ Gender [ ] Male [ ] Female *Necessary to comply with affirmative action-Civil Rights Standard
School Grade ______ (for children only) Custodial parent/guardian____________________________ Phone: _____________________ Cell: __________________ Home address__________________________________________________________________________________________ STREET ADDRESS CITY STATE ZIP
Second parent or guardian or emergency contact_____________________________________ Phone: ________________ Address___________________________________________________________________ Cell: ______________________ STREET ADDRESS CITY STATE ZIP
Emergency contact (someone NOT attending camp): Name ________________________________________________________________________________________________ Relationship _______________________________________________________ Phone: ____________________________ Address__________________________________________________________________ Cell: _______________________ STREET ADDRESS CITY STATE ZIP
Insurance Information Is the participant covered by family medical/hospital insurance? [ ] Yes [ ] No If so, indicate carrier or plan name: ____________________________________________ Group # ___________________ **Photocopy of front and back of health insurance card or current K-chip must be attached to this form.**
General Questions (Explain "yes" answers below.)
Has/does the participant:
Yes Yes No 1. Had any recent injury, illness or infectious disease? 2. Have a chronic or recurring illness/condition? 3. Ever been hospitalized? 4. Ever had surgery? 5. Have frequent headaches? 6. Ever had a head injury? 7. Ever been knocked unconscious? 8. Wear glasses, contacts or protective eye wear? 9. Ever had frequent ear infections? 10. Ever passed out during or after exercise? 11. Ever been dizzy during or after exercise? 12. Ever had an eating disorder? 13. Ever had chest pain during or after exercise? 14. Ever had high blood pressure? 15. Ever been diagnosed with a heart murmur? Please explain any 'yes' answers, noting the number of the
Which of the following has the participant had? [ ] Measles [ ] Chicken Pox [ ] German measles [ ] Mumps [ ] Hepatitis A [ ] Hepatitis B [ ] Hepatitis C TB Mantoux Test Date of last test__________ Result [ ] Positive [ ] Negative [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ [ ] [ questions.
No
[ ] [ ] [ [ [ [ [ [ [ [ [ [ ] ] ] ] ] ] ] ] ] ] [ ] [ ] [ [ [ [ [ [ [ [ [ [ ] ] ] ] ] ] ] ] ] ]
] 16. Ever had back problems? ] 17. Ever had problems with joints; e.g., knees, ankles? ] 18. Have an orthodontic appliance being brought to ] camp? ] 19. Have any skin problems (e.g., itching, rash, acne)? ] 20. If female, have an abnormal menstrual history? ] 21. Had problems with diarrhea/constipation? ] 22. Had mononucleosis in the past 12 months? ] 23. Have diabetes? ] 24. Had problems with sleepwalking? ] 25. Have asthma? ] 26. Have a history of bed-wetting? ] 27. Ever had seizures? ] 28. Ever had emotional difficulties for which ] professional help was sought? __________________________________________
[ ]
[ ]
Please give all dates of immunization for (or attach Vaccine: Dates: Mo/Yr Mo/Yr DTP ______ ______ TD (tetanus/diphtheria) ______ ______ Tetanus ______ ______ Polio ______ ______ MMR ______ ______ or Measles ______ ______ or Mumps ______ ______ or Rubella ______ ______ Haemophilus influenza B ______ ______ Hepatitis B ______ ______ Varicella (chicken pox) ______
official copy from doctors Mo/Yr Mo/Yr ______ ______ ______ ______ ______ ______ ______ ______
office): Mo/Yr ______ ______ ______ ______
Mo/Yr ______ ______ ______ ______
______ ______
______
Health History: The following information must be filled in by the Keep a copy of the completed form for your records. Any changes to this parent -guardian, or adult camper or staff member. The intent of form should be provided to camp health personnel upon participant's arrival this information is to provide camp health care personnel the in camp. Provide complete information so that the camp can be aware of background to provide appropriate care. your needs. ALLERGIES List all known Describe reaction and management of the reaction. Medications allergies (list) _______________________ _______________________________________________________________________________ _______________________ _______________________________________________________________________________ Food allergies (list) _______________________ _____________________________________________________________________________________ _______________________ _____________________________________________________________________________________ Other allergies (list) include insect stings, hay fever, asthma, animal dander, etc. ______________________ _______________________________________________________________________________ ______________________ _______________________________________________________________________________ Please list any DIETARY RESTRICTIONS that apply to this individual.______________________________________________________ _________________________________________________________________________________________________________________
Is there any additional information that camp staff should know to help you/your child be successful and have fun at camp? (behavioral, physical, emotional, special restrictions, etc.) If your child receives medication during the school year, we strongly urge you to keep your child on this medication during camp. __________________________ _______________________________________________________________________________________________________
Name of family physician
_____________
Phone
Address _____ Name of family dentist/orthodontist ____________
__________
Phone
Address __________
For Camp Use Only Date Health Form Reviewed by Camp Medical Personnel: Signature of Reviewer: ___________________________________________________________________
For Military-Extension Adventure Camp Grant Personnel Use Only Date Received:
Dates of Camp Attendance:
Signature:
Important This section must be complete for attendance at any camp!
Parent/Guardian Authorizations: This health history is correct and complete as far as I know. I give permission here in noted to engage in all camp activities except as noted. I hereby give permission to the camp staff to provide routine health care, administer over the counter medications, assist in administering campers prescription medications as needed, and seek emergency medical treatment including ordering x-rays and routine tests. I agree to the release of any records necessary for treatment, referral, billing, or insurance purposes. I give permission to the camp to arrange necessary related transportation for me/my child. In the event I cannot be reached in an emergency, I hereby give permission to the physician selected by the camp to secure and administer treatment, including hospitalization, for the person named above. This completed form may be photocopied for trips out of camp.
Signature of parent/guardian ___________________________________________________ Printed Name ____________________________________ Date: ___________
UNIVERSITY OF KENTUCKY
Camps, Conferences & Field Trips
MEDICAL INSURANCE INFORMATION FORM
Participant Name: Last Address: Street City Participants Social Security No.: Age: Parent/Guardian Name(s): Business phone: Home phone: mother: father: mother: father: step mother: step father: step mother: step father: Date of Birth: State Apt. # Zip Code First Middle I.
Neighbor or Relative (Other than parent/guardian): Phone:
PRIMARY INSURANCE INFORMATION
PARENTS INSURANCE COVERING PARTICIPANT Insured: Policy No.: Insurance Co.: Insurance Co. Address.: SECOND PARENTS INSURANCE (if participant is also covered under this policy) Insured: Policy No.: Insurance Co.: Insurance Co. Address.: 4 Check and sign if participant has no health coverage.
p There is no health insurance coverage for this participant at this time. Signature Parent/Guardian.: Date:
Date of Birth: Member ID #.: Phone #:
Date of Birth: Member ID #.: Phone #:
You MUST submit a copy of the front and back of all insurance and Rx identification cards covering participants.
9
CLEAR PAGE
Insurance Carrier Coverage
CIGNA
Insurance coverage is on an excess basis only. The participants personal health insurance policy will be primary and provide coverage for accident and sickness. The excess policy will cover any out-of-pocket expense not paid by the participants personal insurance up to the limits of the policy listed below. (This includes payment of the deductible and coinsurance amounts if applied under the participants personal policy.) The sickness medical expense will be limited to $500 on an excess basis. The benefit period is one year. The first expense must be incurred within 60 days of the accident or sickness. If the participant does not have personal health insurance coverage, this excess policy will pay first dollar, up to the limits of this policy. Pre-existing conditions are not covered. A pre-existing condition is any condition for which a prudent person should have sought treatment or was treated in the previous six months Accident Medical Expense (Excess) Accident Dental Expense (Excess) Deductible Sickness Medical Expense (Excess) Deductible AD&D and Paralysis, Principal Sum Benefit Period Effective Date Expiration Date Consent to Medical Treatment/Insurance Statement $25,000 Included Nil $500 Nil $10,000 One Year 1/1/11 1/1/12
Coverage Benefits & Limits
It is understood that authority is given to the University of Kentucky, or anyone they may designate, to have my son/daughter treated for injuries or illnesses they incur during a designated camp, conference, or field trip activity at the University of Kentucky. I understand that I will be notified if a health problem arises, but in the event I cannot be reached by telephone, I hereby give the University of Kentucky, or anyone they may designate, permission to seek medical treatment for the participant named below, including surgery (on an emergency basis) or additional advanced treatments (MRI, lab tests, etc.) as deemed necessary by competent medical personnel. I am aware that, as the adult participant, or as the parent or legal guardian of the participant named below, I will be responsible for any expenses incurred outside of the limits provided by the University of Kentuckys Camps/ Conference/Field Trip Policy. I also understand that the University of Kentucky insurance coverage is on an excess basis only. The excess policy will cover any out-of-pocket expense not paid by the participants personal insurance up to the limits of the policy listed above.
____________ Date Name: Phone number: (home) _____________________________ N ame of Participant _________________________________________ Signature (Parent or Guardian if claimant is a minor) Relationship: (work)
Emergency Contact (if other than parent)
10
UNIVERSITY OF KENTUCKY
MEDICAL AUTHORIZATION
AUTHORIZATION TO RELEASE INFORMATION
I authorize any Health Care Provider, Insurance Company, Employer, Person or Organization to release any information regarding medical, dental, mental, alcohol or drug abuse history, treatment or benefits payable, including disability or employment-related information concerning the patient, to any CIGNA company, the Plan administrator or their employees and authorized agents for the purpose of validating and determining benefits payable. This data may be extracted for use in audit or statistical purposes. I understand that I or my authorized representative will receive a copy of this authorization upon request. This authorization or a photostatic copy of the original shall be valid for the duration of the claim.
Signature (Parent or Guardian if claimant is a minor) Date Phone No.
PAYMENT AUTHORIZATION: I authorize all current and future medical benefits, for services rendered and billed as a result of this claim, to be made payable to the physicians and providers indicated on the invoices.
Signature (Parent or Guardian if claimant is a minor) Date
11
12
Military-Extension Adventure Camp Registration Form
Life Adventure Center of the Bluegrass CONSENT AND RELEASE AGREEMENT
*This form must be filled out for EVERY individual participant for every camp EXCEPT the White Water Rafting Trip Participant name (print clearly) _________________________________________________ UK Cooperative Extension/Military Extension Adventure Camp Initiative In consideration of permission to participate in, or continue participating in, the activities and programs of Life Adventure Center of the Bluegrass, and to use its facilities, I hereby acknowledge and agree as follows: I understand that my participation in programs offered by Life Adventure Center of the Bluegrass is purely voluntary. I recognize that the program is designed to use experiential and engaging teaching techniques. At all times, I will choose my level of participation in any activity. Further, I agree that I must comply with requests, directions, and instructions of the individuals offering the programs and my failure to do so may result in my removal from the program. I agree that I will use and wear the appropriate safety equipment. I recognize that my participation in Life Adventure Center of the Bluegrass programs is with some risk of bodily injury. I accept those risks with full knowledge of the dangers involved (including but not limited to: increased heart rate, blood pressure, strained or sprained muscles, fractured bones, partial or complete paralysis, heart attacks, psychological injury, death, or any possibility of serious injury), and hereby certify that I know of no physical or medical problems that would increase my risk of illness or injury, as a result of participating in Life Adventure Center of the Bluegrass programs. I understand that under Kentucky Law a farm animal activity sponsor, farm animal professional, or other person does not have the duty to eliminate all risks of injury of participation in farm animal activities. There are inherent risks of injury that one voluntarily accepts if one participates in farm animal activities. KRS247.4027 In the event of an injury or sudden illness, I consent to the administration of first aid and resuscitative measures performed on my behalf by trained or qualified personnel. I assume full responsibility for all medical expenses incurred as a result of injuries suffered by my participation in Life Adventure Center of the Bluegrass programs. I hereby release and discharge Life Adventure Center of the Bluegrass, its agents, employees, representatives, the building and grounds owners, any related entities, and all others from any and all liability, responsibility, loss, damage, costs, claims, and causes of action
13
(including, but not limited to, those for bodily injury, death, and property damage or loss to me) arising out of or resulting from my use of or presence upon these facilities and/or participation in Life Adventure Center of the Bluegrass programs, specifically including, but not limited to, any and all liability, responsibility, loss, damage, costs, claims, and/or causes of action that arise from or are caused by the negligence or fault of Life Adventure Center of the Bluegrass programs, its agents, employees, representatives, the building and grounds owners, any related entities, or other participants in the Life Adventure Center of the Bluegrass programs. I have read the entire Consent and Release Agreement and accept the conditions stated herein as a requirement for my participation in Life Adventure Center of the Bluegrass programs. PUBLICITY RELEASE: I grant Life Adventure Center of the Bluegrass and persons acting through them, the rights to use, reproduce, assign, and/or distribute photographs, films, videotapes, and sound recordings of myself or my child for use in materials they may create. I release the corporation (photographers, employees, members, and agents) from all debt claims and/or liabilities of any kind whatsoever arising out of my childs appearance in the presentation, the making, or the use of such films or recordings. I hereby waive my right to inspect the finished produce that may be used in connection herewith. Individual names will not be published. I prefer that this participant not have his/her picture taken.
PLEASE READ BEFORE SIGNING _____________________________________________________________________________________ PARTICIPANT SIGNATURE PRINTED NAME AGE EMERGENCY # PARENT/GUARDIAN SIGNATURE (required if under 18): _______________________ DATE__________ Name__________________________ Address ______________________________________________ City____________________ State____ Zip_______ E-mail_____________________________ Phone___________________________
We would like to keep in touch with you! Please give us your address so that we can keep you up to date on future programs and events at LAC. We promise not to bombard your inbox or fill your mailbox with junk. This information will be used for in house purposes only; LAC will not sell or distribute your name or address to any other organization or individuals.
14
Military-Extension Adventure Camp Registration Form
Fort Knox Child, Youth and School Services CONSENT AND RELEASE AGREEMENT *This form PLUS pages 17-24 must be filled out for EVERY individual participant for the White Water Rafting Camp ONLY RELEASE AND INDEMNITY FORM In consideration of the Fort Knox Child, Youth and School Services hosting, staging and sponsoring the UK Cooperative Extension/Military Extension Adventure Camp Initiative and related programs and activities at _____________________(location of camp) from ___________(arrival date) to __________(departure date), we _______________________(name) and _____________________(name), parents/guardians of _________________________(the participant) do hereby on our own behalf and on behalf of our successors, assigns, heirs, executors, personal representatives and administrators: (a) remise, release and forever discharge the Fort Knox Child, Youth and School Services and all of its present and former directors, officers, agents and employees (collectively the Releasees, which term includes their respective successors, heirs, executors and administrators) and do hereby undertake and agree to indemnify and hold harmless the Releasees, from and against all action, suits, loss, damages, rights, claims and demands whatsoever at law or in equity (collectively the Claims) which we may now or hereafter have against the Releasees, or any of them for or by reason of, or in any way arising out of or on account of, all foreseen and unforeseen (and whether or not advised the possibility thereof) bodily and personal injuries (including death) and property damage and all consequences thereof, resulting from or in any way connected, directly or indirectly, with the Participants presence at the Camp and/or the Participants use of the facilities at the Camp and/or the Participants presence at Camp programs and activities not held at camp; (b) undertake and agree to indemnify and hold harmless the Releasees from and against any and all Claims which any third party may now or hereafter have for or any reason of or in any arising out of or on account of, all foreseen and unforeseen bodily and personal injuries (including death) and property damage and all consequences thereof, caused to or incurred or sustained by said third party resulting from or in any way connected, directly and indirectly, with the Participants presence at the Camp; and (c) undertake and agree to indemnify and hold harmless the Releasees form and against all property damage of any kind caused at the Camp or elsewhere, as a result of or in connection with the Camps programs and activities. It is the specific intent and purpose of this instrument to release and discharge any and all claims and causes of action of any kind or nature whatsoever, whether specifically mentioned or no, and the Releaser specifically waives any claim or right to assert that any cause of action, claim or demand or alleged cause of action or claim or demand has been, through oversight or error or intentionally or unintentionally, omitted from this Release and Indemnity. We fully understand the nature of the programs and activities associated with the Camp and inherent risk of bodily and personal injury (including death) resulting hereon.
15
We agree that any violation of the rules of the Camp by the Participant or any behavior that puts the Participant or others at physical or emotional risk will result in immediate dismissal from the Camp at the discretion of the Program Manager or Director of Child, Youth and School Services. In the event we cannot be reached in an emergency, we hereby consent to any medical treatment of the Participant deemed necessary by the medical staff designated by the Program Manager or Director.
PUBLICITY RELEASE: I grant Fort Knox Child, Youth and School Services and persons acting through them, the rights to use, reproduce, assign and/or distribute photographs, films videotapes and sound recordings of Participant for use in materials they may create. I release the Child, Youth and School Services (photographers, employees, members and agents) from all debt claims and/or liabilities of any kind whatsoever arising out of Participants appearance in the presentation, the making, or the use of such films or recordings. I hereby waive my right to inspect the finished product that may be used in connection herewith. Individual names will not be published.
YES, I agree with Publicity Release NO, I do not agree with Publicity Release
We have read and understand the above, and sign below voluntarily. Dated at _________________(City), ______________________(State) This day ___________of___________(month), 20____(year). Parent/Guardian Signature______________________ Witness Signature________________________ Parent/Guardian Signature______________________ Witness Signature________________________ Note: In order for this form to be considered complete, a witness signature MUST accompany each parent/guardian signature.
16
17
18
19
20
21
22
23
24
Você também pode gostar
- Camper App MMDM 2014Documento5 páginasCamper App MMDM 2014omul rosuAinda não há avaliações
- 710 BSB Frsa Flash: For The Week of October 24-28, 2011Documento27 páginas710 BSB Frsa Flash: For The Week of October 24-28, 2011Abbie HammondAinda não há avaliações
- Michigan National Guard Child & Youth Program MonthlyDocumento11 páginasMichigan National Guard Child & Youth Program MonthlyNoscDetroitCommandOmbudsmanAinda não há avaliações
- Bible Camp 2012Documento5 páginasBible Camp 2012Sergeev YuryAinda não há avaliações
- KIDSANDCOPSDocumento2 páginasKIDSANDCOPSprag shahAinda não há avaliações
- Daily Information 04 February 2011Documento2 páginasDaily Information 04 February 2011NicoleAinda não há avaliações
- Daily Info 02 MarchDocumento3 páginasDaily Info 02 MarchNicoleAinda não há avaliações
- Inside 74: Message From Your OmbudsmenDocumento5 páginasInside 74: Message From Your OmbudsmenLesley ClaytonAinda não há avaliações
- Bulletin 4 23 13Documento3 páginasBulletin 4 23 13Michael AllenAinda não há avaliações
- 2011 Summer Camp InfoDocumento6 páginas2011 Summer Camp InfoyoueatmydustAinda não há avaliações
- I Corps Trailblazer Battalion: Weekly NewsDocumento21 páginasI Corps Trailblazer Battalion: Weekly Newsaprilann1980Ainda não há avaliações
- Cabot Panther Sports: Come Out and Support The PanthersDocumento12 páginasCabot Panther Sports: Come Out and Support The Panthersapi-278899289Ainda não há avaliações
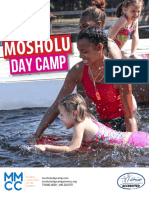
- Camp Brochure 2017Documento7 páginasCamp Brochure 2017Mosholu Montefiore0% (1)
- Family Newsletter HQSVC Co 1 July 2011Documento8 páginasFamily Newsletter HQSVC Co 1 July 20112d Marine Logistics GroupAinda não há avaliações
- Bulletin 3 20 13Documento4 páginasBulletin 3 20 13Michael AllenAinda não há avaliações
- Youth Camp RegistrationDocumento2 páginasYouth Camp RegistrationmiranadhouchinsAinda não há avaliações
- Vance Bulletin 10.27.11Documento2 páginasVance Bulletin 10.27.11EnlistedSpousesAinda não há avaliações
- Cabot Panther Sports: Come Out and Support The PanthersDocumento13 páginasCabot Panther Sports: Come Out and Support The Panthersapi-278899289Ainda não há avaliações
- Cabot Panther Sports: Come Out and Support The PanthersDocumento11 páginasCabot Panther Sports: Come Out and Support The Panthersapi-278899289Ainda não há avaliações
- Bulletin 3 28 13Documento3 páginasBulletin 3 28 13Michael AllenAinda não há avaliações
- Kelly Mill Middle School - March 28th NewsletterDocumento9 páginasKelly Mill Middle School - March 28th NewsletterEmily BoothAinda não há avaliações
- 07-11 Hs FWD Newsletter (Final)Documento8 páginas07-11 Hs FWD Newsletter (Final)Jose PadillaAinda não há avaliações
- MALS News Feb 22 Through Feb 28Documento3 páginasMALS News Feb 22 Through Feb 28mals16Ainda não há avaliações
- Script 2013 02Documento12 páginasScript 2013 02J9 YuAinda não há avaliações
- 2nd Supply Battalion November Family Readiness NewsletterDocumento8 páginas2nd Supply Battalion November Family Readiness NewsletterkfonvilleAinda não há avaliações
- Wu 20130707Documento11 páginasWu 20130707Fred HeitjanAinda não há avaliações
- Akhs Knightly News: Jump Start Recovered Ended Today, Friday, May 3 Recovery Begins On Monday, May 6Documento3 páginasAkhs Knightly News: Jump Start Recovered Ended Today, Friday, May 3 Recovery Begins On Monday, May 6api-198044962Ainda não há avaliações
- School Voluneer FormDocumento1 páginaSchool Voluneer FormMarRoge12Ainda não há avaliações
- Vantage Partner in Regional Grant: Elphos EraldDocumento12 páginasVantage Partner in Regional Grant: Elphos EraldThe Delphos HeraldAinda não há avaliações
- Newsletter 131031Documento2 páginasNewsletter 131031Brian BlankAinda não há avaliações
- GC 08-18 C9 CommunityDocumento1 páginaGC 08-18 C9 CommunityNikki MaxwellAinda não há avaliações
- Bulletin 10 10 13Documento3 páginasBulletin 10 10 13Michael AllenAinda não há avaliações
- Pell City Squadron - Jul 2011Documento14 páginasPell City Squadron - Jul 2011CAP Unit NewslettersAinda não há avaliações
- The Lamppost: Important DatesDocumento14 páginasThe Lamppost: Important DatespazchannelsAinda não há avaliações
- Newsletter 11 10 16Documento2 páginasNewsletter 11 10 16Patrick NolanAinda não há avaliações
- Tallulah High School ReunionDocumento4 páginasTallulah High School Reuniontomrushin9309Ainda não há avaliações
- Camp Bar-V-NokDocumento5 páginasCamp Bar-V-Nokubalim8Ainda não há avaliações
- Browerville Blade - 11/10/2011Documento14 páginasBrowerville Blade - 11/10/2011bladepublishingAinda não há avaliações
- Seahawk ScoopDocumento3 páginasSeahawk ScoopMichael AllenAinda não há avaliações
- Bulletin 11 15 12Documento5 páginasBulletin 11 15 12Michael AllenAinda não há avaliações
- 2014 RegistrationDocumento2 páginas2014 RegistrationevanatubcAinda não há avaliações
- Cabot Panther Sports: Come Out and Support The PanthersDocumento14 páginasCabot Panther Sports: Come Out and Support The Panthersapi-278899289Ainda não há avaliações
- Thunderbolt Jul 2011Documento12 páginasThunderbolt Jul 2011firstroundfamily53Ainda não há avaliações
- Don'T Miss Out On A Week of Spiritual Uplifting and Amazing Adventures!! YW $180Documento5 páginasDon'T Miss Out On A Week of Spiritual Uplifting and Amazing Adventures!! YW $180JenJuddAinda não há avaliações
- Seahawk ScoopDocumento4 páginasSeahawk ScoopMichael AllenAinda não há avaliações
- Cabot Panther Sports: Come Out and Support The PanthersDocumento15 páginasCabot Panther Sports: Come Out and Support The Panthersapi-278899289Ainda não há avaliações
- Bulletin 4 16 13Documento3 páginasBulletin 4 16 13Michael AllenAinda não há avaliações
- Keystone Perry PDJ 8-14-13Documento1 páginaKeystone Perry PDJ 8-14-13Price LangAinda não há avaliações
- Cabot Panther Sports: Come Out and Support The PanthersDocumento13 páginasCabot Panther Sports: Come Out and Support The Panthersapi-278899289Ainda não há avaliações
- Cabot Panther Sports: Come Out and Support The PanthersDocumento11 páginasCabot Panther Sports: Come Out and Support The Panthersapi-278899289Ainda não há avaliações
- Nautical Notes: Principal's ColumnDocumento7 páginasNautical Notes: Principal's Columntica1118Ainda não há avaliações
- Nautical Notes: Principal's ColumnDocumento5 páginasNautical Notes: Principal's Columntica1118Ainda não há avaliações
- Bulletin 11 21 14Documento3 páginasBulletin 11 21 14Michael AllenAinda não há avaliações
- The American Village:: 5th Grade Field TripDocumento16 páginasThe American Village:: 5th Grade Field Tripapi-302045862Ainda não há avaliações
- DH 0610Documento10 páginasDH 0610The Delphos HeraldAinda não há avaliações
- I Corps Trailblazer Battalion: Weekly NewsDocumento24 páginasI Corps Trailblazer Battalion: Weekly Newsaprilann1980Ainda não há avaliações
- Long Distance Relationships GuideDocumento21 páginasLong Distance Relationships GuideAnca Nu0% (2)
- Bison Courier, May 31, 2012Documento20 páginasBison Courier, May 31, 2012surfnewmediaAinda não há avaliações
- What to Expect When Your Child Leaves For College A Complete Guide for Parents OnlyNo EverandWhat to Expect When Your Child Leaves For College A Complete Guide for Parents OnlyAinda não há avaliações
- Daily Information Update 29 March 2011Documento3 páginasDaily Information Update 29 March 2011NicoleAinda não há avaliações
- FRSA Flash - Week Ending 25 March 2011Documento8 páginasFRSA Flash - Week Ending 25 March 2011NicoleAinda não há avaliações
- Daily Information Update 25 August 2011Documento2 páginasDaily Information Update 25 August 2011NicoleAinda não há avaliações
- Frsa Flash - Week Ending 18 March 2011Documento6 páginasFrsa Flash - Week Ending 18 March 2011NicoleAinda não há avaliações
- Daily Information 23 March 2011Documento5 páginasDaily Information 23 March 2011NicoleAinda não há avaliações
- Daily Info 02 MarchDocumento3 páginasDaily Info 02 MarchNicoleAinda não há avaliações
- Daily Information 11 February 2011 With AttachmentsDocumento20 páginasDaily Information 11 February 2011 With AttachmentsNicoleAinda não há avaliações
- Daily Information 04 February 2011Documento2 páginasDaily Information 04 February 2011NicoleAinda não há avaliações
- Daily Information 03 February 2011Documento7 páginasDaily Information 03 February 2011NicoleAinda não há avaliações
- Weekly Overview 12 Jan-19 Jan 2011 (FCW)Documento5 páginasWeekly Overview 12 Jan-19 Jan 2011 (FCW)NicoleAinda não há avaliações
- Obligations and Contracts (Chapter 3 Sec 5)Documento3 páginasObligations and Contracts (Chapter 3 Sec 5)LeeshAinda não há avaliações
- Gulab View Final Tender 27.08.2021Documento37 páginasGulab View Final Tender 27.08.2021Prince RodriguresAinda não há avaliações
- Partnership Withdrawal AgreementDocumento3 páginasPartnership Withdrawal Agreementhuangpeter55Ainda não há avaliações
- Omnibus IndemnityDocumento4 páginasOmnibus IndemnityNitin UpretiAinda não há avaliações
- Sofa For Sale-ManualDocumento13 páginasSofa For Sale-ManualNik FermonAinda não há avaliações
- ITODDocumento8 páginasITODMukesh KumarAinda não há avaliações
- HEIRS OF MARAMAG Vs MARAMAGDocumento2 páginasHEIRS OF MARAMAG Vs MARAMAGjacq17100% (1)
- Designation of A Representative Pursuant To Art. 27 GDPR: 1. Subject Matter of This AgreementDocumento5 páginasDesignation of A Representative Pursuant To Art. 27 GDPR: 1. Subject Matter of This AgreementHoang Tri MinhAinda não há avaliações
- TNB Remaco - Kharafi National JV Attn.: Mohamed Salem Sadat P.O.Box: 24081, Safat - 13101, KuwaitDocumento9 páginasTNB Remaco - Kharafi National JV Attn.: Mohamed Salem Sadat P.O.Box: 24081, Safat - 13101, KuwaitRnldo de CabrioAinda não há avaliações
- Insurance DigestDocumento45 páginasInsurance DigestDenise GordonAinda não há avaliações
- US vs. BernardoDocumento6 páginasUS vs. BernardolictoledoAinda não há avaliações
- Principles of Accounting 11th Edition Needles Solutions ManualDocumento16 páginasPrinciples of Accounting 11th Edition Needles Solutions ManualJamesJacksonnqpf100% (44)
- Kranium Sky 1Documento22 páginasKranium Sky 1joan mukuhaAinda não há avaliações
- DCSD - Acad Final Contract ExecutedDocumento86 páginasDCSD - Acad Final Contract ExecutedSimply SherrieAinda não há avaliações
- Agreement ShopDocumento8 páginasAgreement ShoprahulkishnaniAinda não há avaliações
- Money and Banking (Project Report On Adam Jee Insurance)Documento48 páginasMoney and Banking (Project Report On Adam Jee Insurance)Naveed JuttAinda não há avaliações
- How Are Your Paperwork Headaches?: How To Use This TemplateDocumento10 páginasHow Are Your Paperwork Headaches?: How To Use This TemplatedrixAinda não há avaliações
- B1722 16 FC6AUsersENDocumento662 páginasB1722 16 FC6AUsersENAhmad SolihinAinda não há avaliações
- Philippine Health Care Providers, Inc v. CirDocumento2 páginasPhilippine Health Care Providers, Inc v. CirGretchen CanedoAinda não há avaliações
- JVC Distributor AgreementDocumento11 páginasJVC Distributor AgreementVijay Vardhan KudariAinda não há avaliações
- To Activate Road Side Assistance (RSA) Cover, SMS "ACTIVATE POLICY V7569054 " To 9222211100 (Standard SMS Charges Applicable)Documento9 páginasTo Activate Road Side Assistance (RSA) Cover, SMS "ACTIVATE POLICY V7569054 " To 9222211100 (Standard SMS Charges Applicable)seshu 2010Ainda não há avaliações
- Share and Shareholders Loan Purchase AgreementDocumento5 páginasShare and Shareholders Loan Purchase AgreementLegal Forms100% (1)
- FAQ Saudi Labor Law by AttyChavez PHL Embassy RiyadhDocumento21 páginasFAQ Saudi Labor Law by AttyChavez PHL Embassy RiyadhjonathandacumosAinda não há avaliações
- Test Bank For Anatomy and Physiology 10th Edition by PattonDocumento22 páginasTest Bank For Anatomy and Physiology 10th Edition by Pattonethanmasonbva100% (9)
- Sec. 17 DigestDocumento9 páginasSec. 17 DigestVen John J. LluzAinda não há avaliações
- A8509 - Operation Shelter Security Contract - Final CombinedDocumento7 páginasA8509 - Operation Shelter Security Contract - Final CombinedNBC MontanaAinda não há avaliações
- Sample Producer Contract (Royalty-Bearing Work For Hire)Documento9 páginasSample Producer Contract (Royalty-Bearing Work For Hire)Digital Music News92% (12)
- CORPORATE INTERNET BANKING Form PDFDocumento10 páginasCORPORATE INTERNET BANKING Form PDFМєяяїгг ВєяиндяԁAinda não há avaliações
- Fire InsuranceDocumento3 páginasFire InsuranceAwasthi BrajendraAinda não há avaliações
- CHA vs. Court of AppealsDocumento1 páginaCHA vs. Court of AppealsDonnAinda não há avaliações