Você também pode gostar
- Hearing: An Introduction to Psychological and Physiological AcousticsNo EverandHearing: An Introduction to Psychological and Physiological AcousticsAinda não há avaliações
- FlashcardsDocumento140 páginasFlashcardsDoodAinda não há avaliações
- Otoacoustic Emissions From MedscapeDocumento5 páginasOtoacoustic Emissions From MedscapeMin-Joo Esther ParkAinda não há avaliações
- Audiometric Testing of AdultsDocumento6 páginasAudiometric Testing of AdultssofiameAinda não há avaliações
- Dr. Ashman's ENT Notes PDFDocumento56 páginasDr. Ashman's ENT Notes PDFJulian GordonAinda não há avaliações
- Assessment of HearingDocumento51 páginasAssessment of HearingSwetha PasupuletiAinda não há avaliações
- Basic Audiology (Fred)Documento4 páginasBasic Audiology (Fred)Aisyah BadhrulhishamAinda não há avaliações
- Consultant in Audiology: Passbooks Study GuideNo EverandConsultant in Audiology: Passbooks Study GuideAinda não há avaliações
- Hearing Disorders and Audiogram InterpretationDocumento27 páginasHearing Disorders and Audiogram InterpretationGaluhAinda não há avaliações
- Auditory Brainstem ResponseDocumento18 páginasAuditory Brainstem ResponseFree dataAinda não há avaliações
- Otorhinolaryngology NotesDocumento25 páginasOtorhinolaryngology NotesFako Filipinas100% (3)
- Audiology MaskingDocumento6 páginasAudiology MaskingRavi VarakalaAinda não há avaliações
- Impedance Audiometry - Overview, Indications, ContraindicationsDocumento8 páginasImpedance Audiometry - Overview, Indications, ContraindicationsSorin AilincaiAinda não há avaliações
- Principles of Hearing Aid AudiologyDocumento350 páginasPrinciples of Hearing Aid AudiologybalajiaslpAinda não há avaliações
- A Guide To TympanometryDocumento17 páginasA Guide To Tympanometryoeoe26100% (1)
- Slow Auditory Evoked Potentials (1 InterligneDocumento8 páginasSlow Auditory Evoked Potentials (1 Interligner.boniver524Ainda não há avaliações
- Guideline Hearing Aid FittingDocumento80 páginasGuideline Hearing Aid FittingPhillip Martinez50% (2)
- Speech AudiometryDocumento9 páginasSpeech AudiometryVarunSharmaAinda não há avaliações
- Cholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandCholesteatoma, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Epistaxis (Nose Bleed), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandEpistaxis (Nose Bleed), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- The Acoustic Reflex: Basic Principles and Clinical ApplicationsNo EverandThe Acoustic Reflex: Basic Principles and Clinical ApplicationsShlomo SilmanAinda não há avaliações
- Oae Presentation,/ Kunnampallil GejoDocumento69 páginasOae Presentation,/ Kunnampallil GejoKUNNAMPALLIL GEJO JOHN100% (1)
- Emailing AudiologyDocumento42 páginasEmailing AudiologyIsabel CastilloAinda não há avaliações
- Auditory Brainstem Response - ABR - in Clinical Practice PDFDocumento9 páginasAuditory Brainstem Response - ABR - in Clinical Practice PDFary wisma dewiAinda não há avaliações
- Recurrent Laryngeal Nerve Injury During Thyroidectomy - What NextDocumento31 páginasRecurrent Laryngeal Nerve Injury During Thyroidectomy - What NextAnisur RahmanAinda não há avaliações
- Assessment of HearingDocumento30 páginasAssessment of HearingNitin SharmaAinda não há avaliações
- Genes Hearing DeafnessDocumento328 páginasGenes Hearing DeafnessjvojnicAinda não há avaliações
- Post Laryngectomy Voice RehabilitationDocumento58 páginasPost Laryngectomy Voice RehabilitationfakeywakeyAinda não há avaliações
- Development of An Audiological Test Procedure Manual For First Year Au.D. StudentsDocumento146 páginasDevelopment of An Audiological Test Procedure Manual For First Year Au.D. StudentsThadchai Suwanwarangkool100% (2)
- Larynx Wrote by DR Nassem TalaatDocumento38 páginasLarynx Wrote by DR Nassem TalaatAbouzr Mohammed ElsaidAinda não há avaliações
- LSLS Audiology ProtocolDocumento13 páginasLSLS Audiology ProtocolFebryantiPBundaayabariqAinda não há avaliações
- Facial NerveDocumento68 páginasFacial NerveMédecin Adrian TGAinda não há avaliações
- Audiology Clinic HandbookDocumento81 páginasAudiology Clinic HandbookGilmaria Souza100% (1)
- CSF RhinorrhoeaDocumento12 páginasCSF RhinorrhoeaSuprit Sn100% (5)
- CholesteatomaDocumento29 páginasCholesteatomawhitelotusoo7Ainda não há avaliações
- Mcqs For The DohnsDocumento45 páginasMcqs For The Dohnssaurabhsinghspeaks3543100% (2)
- Assessment of HearingDocumento114 páginasAssessment of Hearinghonda matiz100% (2)
- Cochlear Implantation Technique PDFDocumento9 páginasCochlear Implantation Technique PDFKenric TamAinda não há avaliações
- TympanometryDocumento81 páginasTympanometryastralmaniaAinda não há avaliações
- ASSR Thresholds PDFDocumento7 páginasASSR Thresholds PDFDaniela Garrido GonzálezAinda não há avaliações
- Larynx Removal SurgeryDocumento33 páginasLarynx Removal SurgerySwathi GAinda não há avaliações
- Otosclerosis Slides 061018Documento96 páginasOtosclerosis Slides 061018Paraguay De La Cruz JoelAinda não há avaliações
- (ENT) 1.03 Inner Ear (Part 2) Basic Concepts of Hearing Loss and Aural Rehabilitation - Dr. LagoDocumento7 páginas(ENT) 1.03 Inner Ear (Part 2) Basic Concepts of Hearing Loss and Aural Rehabilitation - Dr. LagoDenise CedeñoAinda não há avaliações
- Glomus TumourDocumento50 páginasGlomus TumourPratibha Goswami100% (1)
- Laryngeal Paralysis - FinalDocumento37 páginasLaryngeal Paralysis - FinalAkanshaAinda não há avaliações
- Physiology of Hearing OtolaryngologyDocumento26 páginasPhysiology of Hearing OtolaryngologyDr.Sherif Bugnah88% (8)
- New Born Hearing FactsDocumento8 páginasNew Born Hearing FactsAhiawortor Kplorla100% (1)
- Assr, Vemp, VNG, OaeDocumento8 páginasAssr, Vemp, VNG, OaeSuprit Sn100% (1)
- Drug Induced Ototoxicity - WDocumento12 páginasDrug Induced Ototoxicity - WsavitageraAinda não há avaliações
- Functional Endoscopic Sinus Surgery (Fess) (3) JDocumento20 páginasFunctional Endoscopic Sinus Surgery (Fess) (3) JJulianthy SuentoAinda não há avaliações
- Auditory Pathway PDFDocumento35 páginasAuditory Pathway PDFJohnson JayarajAinda não há avaliações
- BranchesDocumento350 páginasBranchespmjoshir50% (2)
- Nasal Septal PerforationDocumento13 páginasNasal Septal PerforationDr. T. Balasubramanian75% (4)
- Laryngology NotesDocumento296 páginasLaryngology Notesadham bani younesAinda não há avaliações
- Ent EssaysDocumento78 páginasEnt EssaysNektarios Tsakalos100% (1)
- MS ENT Basic Sciences MGR University September 2009 Question Paper With SolutionDocumento36 páginasMS ENT Basic Sciences MGR University September 2009 Question Paper With SolutionDr. T. Balasubramanian67% (3)
- Temporal Bone Dissection ManualDocumento15 páginasTemporal Bone Dissection Manualabhi2537100% (1)
- US Federal Budget Visualized - Your Tax Dollars at Work PDFDocumento18 páginasUS Federal Budget Visualized - Your Tax Dollars at Work PDFTomás LuisAinda não há avaliações
- Cancer Is A Fungus-Tullio Simoncini MD OncologistDocumento248 páginasCancer Is A Fungus-Tullio Simoncini MD OncologistGianna Barcelli Fantappie100% (2)
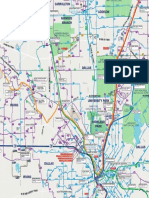
- DARTSystem Map Quad C04 Nov 13Documento1 páginaDARTSystem Map Quad C04 Nov 13Tomás LuisAinda não há avaliações
- XXX Book of Aquarius XXXDocumento163 páginasXXX Book of Aquarius XXXlesgrantonline100% (1)
- XXX Book of Aquarius XXXDocumento163 páginasXXX Book of Aquarius XXXlesgrantonline100% (1)
- Mackie Sr24-4 Sr32-4 OmDocumento67 páginasMackie Sr24-4 Sr32-4 OmbryanvdzAinda não há avaliações
- Numerical Sheet5Documento1 páginaNumerical Sheet5debabratalogonAinda não há avaliações
- Wiring Schematic E19 (S/N AWMM11001 AND ABOVE) (S/N B3LA11001 AND ABOVE) (S/N B3LB11001 AND ABOVE) Sheet 1 of 14Documento14 páginasWiring Schematic E19 (S/N AWMM11001 AND ABOVE) (S/N B3LA11001 AND ABOVE) (S/N B3LB11001 AND ABOVE) Sheet 1 of 14ניקולאי איןAinda não há avaliações
- Omzet 2022Documento177 páginasOmzet 2022Topi Jerami StudioAinda não há avaliações
- LG 55UH8500 CNET Review Calibration ReportDocumento3 páginasLG 55UH8500 CNET Review Calibration ReportDavid KatzmaierAinda não há avaliações
- Abbey Road Saturator: User GuideDocumento10 páginasAbbey Road Saturator: User GuideVianey Macfel TsathyAinda não há avaliações
- Turnigy 9X Service ManualDocumento6 páginasTurnigy 9X Service Manualkrisztiankope100% (2)
- James I. Taylor - The Vibration Analysis Handbook (2003, VCI) - Libgen - Li-19Documento1 páginaJames I. Taylor - The Vibration Analysis Handbook (2003, VCI) - Libgen - Li-19derek brainAinda não há avaliações
- Paleta 2: Lila Rosa Pastel Rosa Celeste Pastel CelesteDocumento4 páginasPaleta 2: Lila Rosa Pastel Rosa Celeste Pastel CelesteLive EvilAinda não há avaliações
- Fancy HotelsDocumento1 páginaFancy HotelsNitesh Kumar PatelAinda não há avaliações
- Crossbones Painting GuideDocumento20 páginasCrossbones Painting GuidelaurentstravaAinda não há avaliações
- Msds Chemical List 2021Documento1 páginaMsds Chemical List 2021Bayu Irawan sgiAinda não há avaliações
- Course 600619110 - Civil Engineering (Sub Group: 0201) Status Government Autonomous Total Seats 10 (MS Seats: 9+ EWS: 1)Documento9 páginasCourse 600619110 - Civil Engineering (Sub Group: 0201) Status Government Autonomous Total Seats 10 (MS Seats: 9+ EWS: 1)Ujwal SaragAinda não há avaliações
- Colour: Pragya Sharma PGT Fine ArtsDocumento15 páginasColour: Pragya Sharma PGT Fine ArtsAnshika GoelAinda não há avaliações
- British Standard Colour ChartDocumento10 páginasBritish Standard Colour ChartMohamed NouzerAinda não há avaliações
- Agamben and Adorno On GestureDocumento9 páginasAgamben and Adorno On GestureLumi MiAinda não há avaliações
- MUE 733 - Week 1 PDFDocumento41 páginasMUE 733 - Week 1 PDFShamimSamsuddinAinda não há avaliações
- Embroidery Principles and Elements of DesignDocumento36 páginasEmbroidery Principles and Elements of DesignEdna NovenoAinda não há avaliações
- Elements of ArtDocumento38 páginasElements of ArtBill Renninger100% (10)
- BHG Colorpersonality Apricot PDFDocumento2 páginasBHG Colorpersonality Apricot PDFMichael KempAinda não há avaliações
- TOP 25 Challenging Puzzles For RRB PO Prelims 2020: Weekly Target (9th August-15th August)Documento16 páginasTOP 25 Challenging Puzzles For RRB PO Prelims 2020: Weekly Target (9th August-15th August)shubham sahuAinda não há avaliações
- Leonard Bernstein: Centennial Logo GuideDocumento9 páginasLeonard Bernstein: Centennial Logo GuideJoao PrezAinda não há avaliações
- X Curve HistoryDocumento6 páginasX Curve HistoryPredrag BlagojevićAinda não há avaliações
- Color PerceptionDocumento11 páginasColor Perceptionrasagna reddyAinda não há avaliações
- SAINT VERONICA LEARNING CENTER CertificateDocumento7 páginasSAINT VERONICA LEARNING CENTER CertificateRandix RAAinda não há avaliações
- Measurement Values: Absolute Color Scales (Available When Display Type Is Absolute)Documento26 páginasMeasurement Values: Absolute Color Scales (Available When Display Type Is Absolute)rafael_dvgAinda não há avaliações
- Stationery CSVDocumento6 páginasStationery CSVFranklin Parra ArzeAinda não há avaliações
- (IISc Lecture Notes 3) M.L. Munjal - Noise and Vibration Control (2013, World Scientific)Documento260 páginas(IISc Lecture Notes 3) M.L. Munjal - Noise and Vibration Control (2013, World Scientific)สาธิต ปริ นทร์ทอง100% (2)
- Dodgson - The Language of Color WheelsDocumento14 páginasDodgson - The Language of Color WheelsGuilherme BiancarelliAinda não há avaliações
- Perfume Is A Liquid That Gives People, Things and Rooms A GoodDocumento4 páginasPerfume Is A Liquid That Gives People, Things and Rooms A GoodAdhe NovyAinda não há avaliações