Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Federal Trade Commission PBM Model OrderDocumento27 páginasFederal Trade Commission PBM Model OrderHelen BennettAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- What Living As A Resident Can Teach Long-Term Care Staff: The Power of Empathy To Transform Care (Excerpt)Documento14 páginasWhat Living As A Resident Can Teach Long-Term Care Staff: The Power of Empathy To Transform Care (Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.Ainda não há avaliações
- Health Insurance Fronter Script 3.5Documento3 páginasHealth Insurance Fronter Script 3.5Jolly Silastre100% (2)
- ScriptDocumento3 páginasScriptEnrico Cayme100% (8)
- Stipulation and OrderDocumento3 páginasStipulation and OrderGrant BosseAinda não há avaliações
- Archaeus 4Documento107 páginasArchaeus 4terrythecensorAinda não há avaliações
- College of Nursing East Coast Institute of Medical Sciences, PondicherryDocumento16 páginasCollege of Nursing East Coast Institute of Medical Sciences, PondicherryRuby Sri100% (1)
- Dred - Bald Mileage EstimateDocumento1 páginaDred - Bald Mileage EstimateGrant BosseAinda não há avaliações
- Plaintiff's Objection To Defendant's Motion To DismissDocumento23 páginasPlaintiff's Objection To Defendant's Motion To DismissGrant BosseAinda não há avaliações
- Balboni Letter - Charter Schools 10-10-12Documento3 páginasBalboni Letter - Charter Schools 10-10-12Grant BosseAinda não há avaliações
- Fitch Bond Statement On NH GO Bond Sale 10-18-2011Documento3 páginasFitch Bond Statement On NH GO Bond Sale 10-18-2011Grant BosseAinda não há avaliações
- Peterson Affidavit in Support of ObjectionDocumento3 páginasPeterson Affidavit in Support of ObjectionGrant BosseAinda não há avaliações
- Objection To Motion For Preliminary InjunctionDocumento3 páginasObjection To Motion For Preliminary InjunctionGrant BosseAinda não há avaliações
- MTD MolDocumento12 páginasMTD MolGrant Bosse100% (1)
- Carrier Affidavit in Support of ObjectionDocumento2 páginasCarrier Affidavit in Support of ObjectionGrant BosseAinda não há avaliações
- Telemedicine After The COVID-19Documento61 páginasTelemedicine After The COVID-19ZAinda não há avaliações
- Cambridge University Press, The Society For Healthcare Epidemiology of America Infection Control and Hospital EpidemiologyDocumento24 páginasCambridge University Press, The Society For Healthcare Epidemiology of America Infection Control and Hospital EpidemiologyCarissa SulaimanAinda não há avaliações
- Swander Final Teaching PlanDocumento16 páginasSwander Final Teaching Planapi-259047759Ainda não há avaliações
- Weirich7e CasesDocumento18 páginasWeirich7e Casescuwekaza0% (1)
- Audit Planning: SGB & CDocumento17 páginasAudit Planning: SGB & CMelanie SamsonaAinda não há avaliações
- Times Leader 08-18-2012Documento56 páginasTimes Leader 08-18-2012The Times LeaderAinda não há avaliações
- OBH G FormDocumento52 páginasOBH G FormRMAinda não há avaliações
- Interim Report: Fraud and Error in Virginia's Medicaid ProgramDocumento81 páginasInterim Report: Fraud and Error in Virginia's Medicaid ProgramBeverly TranAinda não há avaliações
- Full Administrative Medical Assisting 8Th Edition French Solutions Manual PDF Docx Full Chapter ChapterDocumento36 páginasFull Administrative Medical Assisting 8Th Edition French Solutions Manual PDF Docx Full Chapter Chapterligsamcathodic.ovcb100% (26)
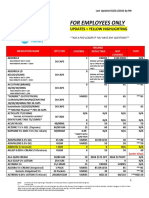
- Employee Only Pricing Sheet 02.11.22Documento10 páginasEmployee Only Pricing Sheet 02.11.22rickyAinda não há avaliações
- Tues., July 26, 2011Documento10 páginasTues., July 26, 2011The Delphos HeraldAinda não há avaliações
- Cooper Et Al., 2022 Geographical Variation in Health Spending Across The US Among Privately InsuredDocumento11 páginasCooper Et Al., 2022 Geographical Variation in Health Spending Across The US Among Privately InsuredDayn KirkseyAinda não há avaliações
- MedEnroll PECOS ProviderSup FactSheet ICN903767Documento14 páginasMedEnroll PECOS ProviderSup FactSheet ICN903767Bishyer AmitAinda não há avaliações
- Obamacare A Step BackwardsDocumento2 páginasObamacare A Step BackwardsGerardFVAinda não há avaliações
- Digest Insurance Fortune Medicare, Inc V Amorin, GR 195872, MArch 12, 2014Documento1 páginaDigest Insurance Fortune Medicare, Inc V Amorin, GR 195872, MArch 12, 2014reiAinda não há avaliações
- Upper Bucks Free Press - September 2013Documento20 páginasUpper Bucks Free Press - September 2013Christopher BetzAinda não há avaliações
- Hospice Care NursingDocumento23 páginasHospice Care NursingLee BuelaAinda não há avaliações
- Annual Report 2010Documento56 páginasAnnual Report 2010amatamesAinda não há avaliações
- Notice: Medicare and Medicaid: Program Issuances and Coverage Decisions Quarterly ListingDocumento41 páginasNotice: Medicare and Medicaid: Program Issuances and Coverage Decisions Quarterly ListingJustia.comAinda não há avaliações
- Remote Therapeutic Monitoring For 2022: Barbara Frances Kho, RN MANDocumento12 páginasRemote Therapeutic Monitoring For 2022: Barbara Frances Kho, RN MANBFKHOAinda não há avaliações
- Premium Support in MedicareDocumento4 páginasPremium Support in MedicareAi NurcahyaniAinda não há avaliações
- Do Certificate-of-Need Laws Increase Indigent Care?Documento32 páginasDo Certificate-of-Need Laws Increase Indigent Care?Mercatus Center at George Mason UniversityAinda não há avaliações
- OHP HandbookDocumento40 páginasOHP HandbookraAinda não há avaliações
- The Complete HSA GuidebookDocumento229 páginasThe Complete HSA GuidebookMichelle LumAinda não há avaliações