Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Tx. COVID 19 en UCIDocumento6 páginasTx. COVID 19 en UCIVictor Augusto Ávila HernándezAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Ghid de Resuscitare Dupa Chirurgia Cardiaca EACTS 2009Documento24 páginasGhid de Resuscitare Dupa Chirurgia Cardiaca EACTS 2009Raluca L100% (1)
- Surgical Reconstruction of Interdental Papilla Using Subepithelialconnective Tissue Graft by Microsurgical Technique A Clinical ST 2376 032X 1000229Documento6 páginasSurgical Reconstruction of Interdental Papilla Using Subepithelialconnective Tissue Graft by Microsurgical Technique A Clinical ST 2376 032X 1000229neighAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Language of AnatomyDocumento7 páginasThe Language of AnatomyLinziJaeOnelAinda não há avaliações
- 03 Anaesthesia Machine PDFDocumento0 página03 Anaesthesia Machine PDFjuniorebindaAinda não há avaliações
- What To Do About Extracranial and Intracranial Stenosis: Home About Issues Categories Back Issues Case Reports ContactDocumento13 páginasWhat To Do About Extracranial and Intracranial Stenosis: Home About Issues Categories Back Issues Case Reports ContactpramitaListyAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Foundation Module Embrology and Gernal Anatomy MCQ by DR of 2027 28Documento53 páginasFoundation Module Embrology and Gernal Anatomy MCQ by DR of 2027 28Xandws -IOS tips and trick and gamingAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
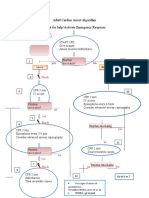
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocumento1 páginaAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Rhinoplasty With Barbed Threads: CosmeticDocumento12 páginasRhinoplasty With Barbed Threads: CosmeticRaphaela TravassosAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Catalogo Dtek NylonDocumento25 páginasCatalogo Dtek NylonAna UmañaAinda não há avaliações
- Assem Draz: Neurological DisordersDocumento26 páginasAssem Draz: Neurological DisordersxuexueAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Surgery For Endocrinological Diseases and Malformations in ChildhoodDocumento155 páginasSurgery For Endocrinological Diseases and Malformations in ChildhoodBeng DinAinda não há avaliações
- Final Physical ExaminationDocumento3 páginasFinal Physical Examinationapi-620159117Ainda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- EZ-IO Insertion Proximal Humerus - in DepthDocumento36 páginasEZ-IO Insertion Proximal Humerus - in Depthwps013100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Basic Life Support: Elements of The Survey The SceneDocumento5 páginasBasic Life Support: Elements of The Survey The SceneMarrianne MortaAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Gastro EndosDocumento263 páginasGastro EndosJay Seetohul50% (2)
- How I Bypassed My Bypass-SurgeryDocumento4 páginasHow I Bypassed My Bypass-Surgeryharinag49Ainda não há avaliações
- Ix - (Revised) Med Cert ValidationDocumento5 páginasIx - (Revised) Med Cert ValidationAlvin Xtian NucumAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Performing Different Types of BiopsiesDocumento5 páginasPerforming Different Types of BiopsiesTALHA AKRAMAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Worksheets - Isbar 3 StrokeDocumento3 páginasWorksheets - Isbar 3 Strokeapi-673621869Ainda não há avaliações
- Sdfa Sdfasdk JFLKSDF Asdfasdf Sdaf AsdfDocumento19 páginasSdfa Sdfasdk JFLKSDF Asdfasdf Sdaf AsdfFaris BariqiAinda não há avaliações
- Emergency Profile ManagementDocumento13 páginasEmergency Profile ManagementCristian PazAinda não há avaliações
- Anal GlandsDocumento7 páginasAnal GlandsSuraj_Subedi100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- VaricoceleDocumento10 páginasVaricoceleDenny SetyadiAinda não há avaliações
- Rsi Currency Practical 3 1Documento2 páginasRsi Currency Practical 3 1Cristian CoronelAinda não há avaliações
- Https Emedicine - MedscapeDocumento14 páginasHttps Emedicine - MedscapeNanaAinda não há avaliações
- Lung Cancer Case Study 4Documento36 páginasLung Cancer Case Study 4mulanAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Shoulder CodeDocumento2 páginasShoulder CodeNasfikurAinda não há avaliações
- AngiotechDocumento48 páginasAngiotechWei LiangAinda não há avaliações
- Guide To Dental Treatment BandsDocumento2 páginasGuide To Dental Treatment BandsVikram Kapur100% (1)