Você também pode gostar
- Infectious Diseases: Smart Study Guide for Medical Students, Residents, and Clinical ProvidersNo EverandInfectious Diseases: Smart Study Guide for Medical Students, Residents, and Clinical ProvidersAinda não há avaliações
- OS MRSA Gostev 2023Documento9 páginasOS MRSA Gostev 2023aiturraldeAinda não há avaliações
- Composite SCC Mec Element in Single-Locus Variant (ST217) of Epidemic MRSA-15 CloneDocumento3 páginasComposite SCC Mec Element in Single-Locus Variant (ST217) of Epidemic MRSA-15 CloneMark ReinhardtAinda não há avaliações
- JCDR 7 1339Documento4 páginasJCDR 7 1339RahayuAinda não há avaliações
- Antibiotics and Animals 2010Documento15 páginasAntibiotics and Animals 2010GARY FRENCHAinda não há avaliações
- MecC VitekDocumento3 páginasMecC VitekmotibaAinda não há avaliações
- Himartshu MethodDocumento5 páginasHimartshu MethodNiveditha NagasundaramAinda não há avaliações
- Van B Positive Vancomycin - Resistant Staphylococcus Aureus Among Clinical Isolates in Shendi City, Northern SudanDocumento5 páginasVan B Positive Vancomycin - Resistant Staphylococcus Aureus Among Clinical Isolates in Shendi City, Northern SudanInternational Organization of Scientific Research (IOSR)Ainda não há avaliações
- Journal of Clinical Immunology & MicrobiologyDocumento9 páginasJournal of Clinical Immunology & MicrobiologyAthenaeum Scientific PublishersAinda não há avaliações
- Journal of Infection and Chemotherapy: SciencedirectDocumento4 páginasJournal of Infection and Chemotherapy: SciencedirectRaodatul IstiharohAinda não há avaliações
- Prevalence of Methicillinresistant Staphylococcus Aureus Andor Intermediate Susceptibility To Vancomycin Isolated From PDocumento7 páginasPrevalence of Methicillinresistant Staphylococcus Aureus Andor Intermediate Susceptibility To Vancomycin Isolated From Pعالمي الجميلAinda não há avaliações
- Due To Two Methicillin-Resistant Widespread Skin and Soft-Tissue InfectionsDocumento7 páginasDue To Two Methicillin-Resistant Widespread Skin and Soft-Tissue Infectionschilvys04Ainda não há avaliações
- J. Clin. Microbiol. 2011 Shi 1972 4Documento3 páginasJ. Clin. Microbiol. 2011 Shi 1972 4we sagara dewiAinda não há avaliações
- Characteristics of Community-And Hospital - Acquired Meticillin-Resistant Staphylococcus Aureus Strains Carrying Sccmec Type Iv Isolated in MalaysiaDocumento6 páginasCharacteristics of Community-And Hospital - Acquired Meticillin-Resistant Staphylococcus Aureus Strains Carrying Sccmec Type Iv Isolated in Malaysiabenny christantoAinda não há avaliações
- 5.4 Risk Factors For MRSA ColonizationDocumento8 páginas5.4 Risk Factors For MRSA ColonizationQworldAinda não há avaliações
- A New Multiplex PCR-based Reverse Line-Blot Hybridization (MPCR-RLB) Assay For Rapid Staphylococcal Cassette Chromosome Mec (SCCmec) TypingDocumento13 páginasA New Multiplex PCR-based Reverse Line-Blot Hybridization (MPCR-RLB) Assay For Rapid Staphylococcal Cassette Chromosome Mec (SCCmec) Typingrajeshkundapur123Ainda não há avaliações
- S AureusDocumento8 páginasS AureusMario Andres Quezada AguiluzAinda não há avaliações
- Journal of Clinical Microbiology-2008-Currie-3101.fullDocumento3 páginasJournal of Clinical Microbiology-2008-Currie-3101.fullMai BasionyAinda não há avaliações
- Molecular EpidemiologyDocumento11 páginasMolecular EpidemiologymotibaAinda não há avaliações
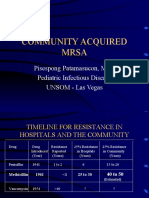
- Community Acquired Mrsa: Pisespong Patamasucon, M.D. Pediatric Infectious Disease UNSOM - Las VegasDocumento48 páginasCommunity Acquired Mrsa: Pisespong Patamasucon, M.D. Pediatric Infectious Disease UNSOM - Las VegasRashed NazzalAinda não há avaliações
- 1 s2.0 S1201971220308407 MainDocumento2 páginas1 s2.0 S1201971220308407 MainАня МурзаковаAinda não há avaliações
- 1 s2.0 S0882401023003340 MainDocumento10 páginas1 s2.0 S0882401023003340 MainEzekiel GreenAinda não há avaliações
- 2011 Cuny MecCDocumento5 páginas2011 Cuny MecCAmanda SilvaAinda não há avaliações
- Staphylococcus Aureus: Antiseptic Resistance Gene Distribution Antimicrobial Agent of Susceptibilities andDocumento8 páginasStaphylococcus Aureus: Antiseptic Resistance Gene Distribution Antimicrobial Agent of Susceptibilities andRisna IrvianiAinda não há avaliações
- AaronDocumento24 páginasAaronCristhian Jover CastroAinda não há avaliações
- Articulo Evaluacion Final Antimicrobianos 1 2020Documento9 páginasArticulo Evaluacion Final Antimicrobianos 1 2020Juan BojacaAinda não há avaliações
- Staphylococcus Aureus in Dermatology Outpatients With Special Emphasis On Community-Associated Methicillin-Resistant StrainsDocumento10 páginasStaphylococcus Aureus in Dermatology Outpatients With Special Emphasis On Community-Associated Methicillin-Resistant StrainsNazihan Safitri AlkatiriAinda não há avaliações
- Increased Vancomycin Mics For Staphylococcus Aureus Clinical Isolates From A University Hospital During A 5-Year PeriodDocumento4 páginasIncreased Vancomycin Mics For Staphylococcus Aureus Clinical Isolates From A University Hospital During A 5-Year Periodbarreiros8Ainda não há avaliações
- Saureus Meti RDocumento6 páginasSaureus Meti RShi-Long LoiAinda não há avaliações
- Antimicrobial Agents and Chemotherapy 2006 Ojo 1089.fullDocumento3 páginasAntimicrobial Agents and Chemotherapy 2006 Ojo 1089.fullJeks VSAinda não há avaliações
- 236 - Spectral Karyotyping of The Human Colon Cancer Cell Lines SW480 and SW620Documento8 páginas236 - Spectral Karyotyping of The Human Colon Cancer Cell Lines SW480 and SW620Fran MoyaAinda não há avaliações
- Dfa 5 23575Documento4 páginasDfa 5 23575Dayat Muh DacilAinda não há avaliações
- J ImmunolDocumento10 páginasJ ImmunolCanda ArdityaAinda não há avaliações
- Osteomyelitis JournalDocumento7 páginasOsteomyelitis JournalAmalia Dwi AryantiAinda não há avaliações
- Review of Related LiteratureDocumento4 páginasReview of Related Literaturegaius avvaAinda não há avaliações
- MrsaDocumento10 páginasMrsazia ul RahmanAinda não há avaliações
- Antimicrob. Agents Chemother. 2006 Chongtrakool 1001 12Documento13 páginasAntimicrob. Agents Chemother. 2006 Chongtrakool 1001 12rahmawati aliwarmanAinda não há avaliações
- Research Paper On MrsaDocumento4 páginasResearch Paper On Mrsam0d1p1fuwub2100% (1)
- Determibation of Bacterial Load by Real Time PCR Using A Broad Range Universal Probeand Primers SetDocumento10 páginasDetermibation of Bacterial Load by Real Time PCR Using A Broad Range Universal Probeand Primers SetYue Ichiban-jō No AneAinda não há avaliações
- Fda ST398Documento30 páginasFda ST398ophexus1205Ainda não há avaliações
- Meticillin Resistant - Staphylococcus - Aure20160520 7685 19p6anl With Cover Page v2Documento11 páginasMeticillin Resistant - Staphylococcus - Aure20160520 7685 19p6anl With Cover Page v2Delvita ElyasAinda não há avaliações
- Mscano, Layout Editor, Jidc-011-0513Documento4 páginasMscano, Layout Editor, Jidc-011-0513dary.podoliak03Ainda não há avaliações
- Microbial Pathogenesis: SciencedirectDocumento8 páginasMicrobial Pathogenesis: SciencedirectMaria Silvana AlvesAinda não há avaliações
- Oxacillin Resistant Staphylococcus Aureus Among Hiv Infected and Non-Infected Kenyan PatientsDocumento8 páginasOxacillin Resistant Staphylococcus Aureus Among Hiv Infected and Non-Infected Kenyan PatientsRina ErlinaAinda não há avaliações
- JM 002170Documento4 páginasJM 002170carmen quispeAinda não há avaliações
- Staphylococcus Aureus Carrying Mecc Gene in Animals and Urban Wastewater, SpainDocumento3 páginasStaphylococcus Aureus Carrying Mecc Gene in Animals and Urban Wastewater, SpainMark ReinhardtAinda não há avaliações
- 1 s2.0 S0956713516300160 MainDocumento8 páginas1 s2.0 S0956713516300160 MainRizkaAinda não há avaliações
- SAP PaperDocumento8 páginasSAP PapertdgioiAinda não há avaliações
- Salmonella Typhi 2012Documento60 páginasSalmonella Typhi 2012Mohd Syaiful Mohd ArisAinda não há avaliações
- Reviews: Methicillin-Resistant Staphylococcus: An Overview of Basic and Clinical ResearchDocumento16 páginasReviews: Methicillin-Resistant Staphylococcus: An Overview of Basic and Clinical ResearchAch Ri Fa IAinda não há avaliações
- Prevalence and Antimicrobial Resistance Pattern of Methicillin Resistant Staphylococcus Aureus (MRSA) Strains..Documento7 páginasPrevalence and Antimicrobial Resistance Pattern of Methicillin Resistant Staphylococcus Aureus (MRSA) Strains..Andi EsSeAinda não há avaliações
- Infectious Diseases: Molecular Characteristics and Virulence Gene Profiles of Causing Bloodstream InfectionDocumento8 páginasInfectious Diseases: Molecular Characteristics and Virulence Gene Profiles of Causing Bloodstream InfectionyutefupAinda não há avaliações
- Mssa 2011 PDFDocumento8 páginasMssa 2011 PDFBebenzzzAinda não há avaliações
- Current Concepts On The Virulence Mechanisms of Meticillin-Resistant Staphylococcus AureusDocumento15 páginasCurrent Concepts On The Virulence Mechanisms of Meticillin-Resistant Staphylococcus AureusSeptiani HasibuanAinda não há avaliações
- Antibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHDocumento5 páginasAntibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHzia ul RahmanAinda não há avaliações
- The Menace of MRSADocumento51 páginasThe Menace of MRSArsborromeoAinda não há avaliações
- MrsaDocumento63 páginasMrsaRAHULAinda não há avaliações
- Diagnosis of Bacteriuria and Leukocyturia by Automated Flow Cytometry Compared With Urine CultureDocumento7 páginasDiagnosis of Bacteriuria and Leukocyturia by Automated Flow Cytometry Compared With Urine CultureAriHendraWijayantiAinda não há avaliações
- Antibiotic Resistant Bacteria in Hospital Wastewaters and Sewage Treatment PlantsDocumento5 páginasAntibiotic Resistant Bacteria in Hospital Wastewaters and Sewage Treatment Plantstoko pojokAinda não há avaliações
- 10 Rights in Drug AdministrationDocumento25 páginas10 Rights in Drug AdministrationNathaniel PulidoAinda não há avaliações
- Daily Newspaper - 2015 - 11 - 09 - 000000Documento54 páginasDaily Newspaper - 2015 - 11 - 09 - 000000Anonymous QRT4uuQAinda não há avaliações
- Catatonia PDFDocumento9 páginasCatatonia PDFDanilo RibeiroAinda não há avaliações
- NCPDocumento8 páginasNCPDoneva Lyn MedinaAinda não há avaliações
- Cardiac Monitoring PDFDocumento7 páginasCardiac Monitoring PDFDelia LopAinda não há avaliações
- NCP TractionDocumento9 páginasNCP TractionAnneSitjar100% (1)
- Zentel Tablets: What Is in This LeafletDocumento3 páginasZentel Tablets: What Is in This LeafletLadyKahluaAinda não há avaliações
- Ranitidine 50mg - 2ml Solution For Injection and Infusion - (EMC) Print FriendlyDocumento6 páginasRanitidine 50mg - 2ml Solution For Injection and Infusion - (EMC) Print FriendlyDewi Wara ShintaAinda não há avaliações
- Cardiovascular Physiology Case 9Documento50 páginasCardiovascular Physiology Case 9Kim AcostaAinda não há avaliações
- Medical Care of Patients With External FixatorDocumento16 páginasMedical Care of Patients With External FixatorStella GašparušAinda não há avaliações
- Clinical Peer Review Literature ExcerptsDocumento4 páginasClinical Peer Review Literature ExcerptsCao Minh TríAinda não há avaliações
- Crit Care Nurse 2011 Grossbach 30 44Documento18 páginasCrit Care Nurse 2011 Grossbach 30 44Hanik FiriaAinda não há avaliações
- 10 1016@j Lungcan 2016 10 008Documento2 páginas10 1016@j Lungcan 2016 10 008restu anindityaAinda não há avaliações
- Root BiomodificationDocumento56 páginasRoot BiomodificationDr Jinal Desai50% (2)
- Bell''s PalsyDocumento54 páginasBell''s Palsywahyu_sitaAinda não há avaliações
- Management of Severe Hyperkalemia PDFDocumento6 páginasManagement of Severe Hyperkalemia PDFCarlos Navarro YslaAinda não há avaliações
- Breathing DifficultyDocumento13 páginasBreathing DifficultygivamathanAinda não há avaliações
- Radioactive Iodine Therapy (Rai) : GoalsDocumento6 páginasRadioactive Iodine Therapy (Rai) : GoalsFirras SalsabilaAinda não há avaliações
- What Is A Case Study?: Roberta Heale, Alison TwycrossDocumento2 páginasWhat Is A Case Study?: Roberta Heale, Alison TwycrossBianca Benj ZariAinda não há avaliações
- QC Delta PV PPT Student 09Documento8 páginasQC Delta PV PPT Student 09Susianna RismandaAinda não há avaliações
- Board Exam QuestionsDocumento2 páginasBoard Exam Questionsgodwinkent888Ainda não há avaliações
- Pathophysiology of FractureDocumento2 páginasPathophysiology of FractureVenus Tagaan UcatAinda não há avaliações
- Proximal Stripping PDFDocumento11 páginasProximal Stripping PDFsmilecarekkmAinda não há avaliações
- Cardio DrillDocumento24 páginasCardio DrillDemuel Dee L. BertoAinda não há avaliações
- Danielle Armour Resume 2017Documento1 páginaDanielle Armour Resume 2017daniellearmour24Ainda não há avaliações
- Support Services SOPDocumento18 páginasSupport Services SOPdamarwuAinda não há avaliações
- Acute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoDocumento20 páginasAcute Pancreatitis: Aguirre, Lucas Galligani, Guido Gorostiaga, Marcos Kreutzer, GustavoGüids GalliganiAinda não há avaliações
- Operational Forces Medical Liaison: Office InformationDocumento4 páginasOperational Forces Medical Liaison: Office InformationRicky PermataAinda não há avaliações
- Article PDF Neeraj Madan Nidhi Kathuria 49Documento3 páginasArticle PDF Neeraj Madan Nidhi Kathuria 49evieramawati_4536812Ainda não há avaliações
- EMG Assisted Migraine TherapyDocumento6 páginasEMG Assisted Migraine TherapyTaufeeq Malik100% (1)