Você também pode gostar
- MRN: - Weight: - KG AgeDocumento2 páginasMRN: - Weight: - KG AgeElaina Gonçalves Silva FurlanAinda não há avaliações
- OBSTETRIC ASSESSMENT TOOLDocumento5 páginasOBSTETRIC ASSESSMENT TOOLDud AccAinda não há avaliações
- Registration FormDocumento5 páginasRegistration FormSreejith Kelakam100% (1)
- List of Employees, Their Duties & Responsibilities Chief of Hospital-IiDocumento4 páginasList of Employees, Their Duties & Responsibilities Chief of Hospital-IiCharisse WooAinda não há avaliações
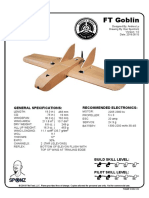
- FT Goblin Full SizeDocumento7 páginasFT Goblin Full SizeDeakon Frost100% (1)
- Ambulatory Care Medical Surgical NursingDocumento11 páginasAmbulatory Care Medical Surgical NursingNiña Antoniette Gutang100% (4)
- Emergency Room Assessment Form: Best Eye Opening Best VerbalDocumento2 páginasEmergency Room Assessment Form: Best Eye Opening Best Verbaleliza marie luisAinda não há avaliações
- 3DS MAX SYLLABUSDocumento8 páginas3DS MAX SYLLABUSKannan RajaAinda não há avaliações
- Clinical Audit On Wastage of Blood ComponentsDocumento30 páginasClinical Audit On Wastage of Blood ComponentsPrabhat KumarAinda não há avaliações
- Preceptor EvaluationDocumento2 páginasPreceptor Evaluationapi-380898658Ainda não há avaliações
- Riaz Gul AHN Unit 1Documento106 páginasRiaz Gul AHN Unit 1Riaz Gul RindAinda não há avaliações
- QSK45 60 oil change intervalDocumento35 páginasQSK45 60 oil change intervalHingga Setiawan Bin SuhadiAinda não há avaliações
- Western Australian Patient Identification Policy PDFDocumento14 páginasWestern Australian Patient Identification Policy PDFpuspadiniaAinda não há avaliações
- Prof. Maria Susan Z. MaglaquiDocumento24 páginasProf. Maria Susan Z. MaglaquiSusan MaglaquiAinda não há avaliações
- Entrepreneurship WholeDocumento20 páginasEntrepreneurship WholeKrizztian SiuaganAinda não há avaliações
- DSA NotesDocumento87 páginasDSA NotesAtefrachew SeyfuAinda não há avaliações
- Category Health Workers PDFDocumento37 páginasCategory Health Workers PDFAparna Kingini100% (1)
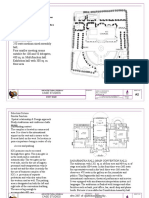
- International Convention Center, BanesworDocumento18 páginasInternational Convention Center, BanesworSreeniketh ChikuAinda não há avaliações
- En - PPR - Nursing College & School of NursingDocumento129 páginasEn - PPR - Nursing College & School of NursingDonor CrewAinda não há avaliações
- Banas Dairy ETP Training ReportDocumento38 páginasBanas Dairy ETP Training ReportEagle eye0% (2)
- A&E Triage SystemDocumento5 páginasA&E Triage SystemArnel AlmutiahAinda não há avaliações
- Safe Injection Practices and Handling of SharpsDocumento26 páginasSafe Injection Practices and Handling of SharpsbrightyAinda não há avaliações
- CCUDocumento82 páginasCCUSarah100% (1)
- Annual Plan: Infection Prevention & Control DepartmentDocumento3 páginasAnnual Plan: Infection Prevention & Control DepartmentSherina Edding0% (1)
- OSCE Station 1 Diabetic LL ExamDocumento5 páginasOSCE Station 1 Diabetic LL ExamJeremy YangAinda não há avaliações
- The Canadian Triage and Acuity Scale: Education Manual: Version 2.5, 2012Documento38 páginasThe Canadian Triage and Acuity Scale: Education Manual: Version 2.5, 2012abdullahmushlihAinda não há avaliações
- World Heart Day 2011: One World, One Home, One HeartDocumento35 páginasWorld Heart Day 2011: One World, One Home, One HeartSoikotAinda não há avaliações
- Needle Stick InjuryDocumento19 páginasNeedle Stick InjuryPRADIPAinda não há avaliações
- Admission and EmergencyDocumento12 páginasAdmission and EmergencyRashid AyubiAinda não há avaliações
- A3 - Lamination - 2Documento10 páginasA3 - Lamination - 2mindmade brandingAinda não há avaliações
- Health Administration Levels, DepartmentsDocumento10 páginasHealth Administration Levels, DepartmentsjessyAinda não há avaliações
- EHRIG - Vol1 - Final Ethiopia Wond G PDFDocumento400 páginasEHRIG - Vol1 - Final Ethiopia Wond G PDFNasradin AhmedAinda não há avaliações
- HDFCLife Little Book of LegacyDocumento18 páginasHDFCLife Little Book of LegacyNaresh KewalramaniAinda não há avaliações
- SYLLABUS Nurse Grade-II ExamDocumento3 páginasSYLLABUS Nurse Grade-II ExamDivyesh PatelAinda não há avaliações
- Critical Care Update PDFDocumento25 páginasCritical Care Update PDFHugo PozoAinda não há avaliações
- LeptospirosisDocumento12 páginasLeptospirosisKim NichiAinda não há avaliações
- MedicineDocumento19 páginasMedicineSarah100% (1)
- Bangladesh National Health Policy-2011Documento19 páginasBangladesh National Health Policy-2011Fairouz Khan100% (1)
- 05 Developing Standards ofDocumento8 páginas05 Developing Standards ofSachin SinghAinda não há avaliações
- Australian Model Triage ScaleDocumento3 páginasAustralian Model Triage ScaleHendraDarmawanAinda não há avaliações
- Major Health Problems in IndiaDocumento5 páginasMajor Health Problems in IndiaVallesh Shetty0% (1)
- Orientation Booklet For Emergency DepartmentDocumento10 páginasOrientation Booklet For Emergency Departmentshahidchaudhary100% (1)
- Oral Health 1-3&5Documento38 páginasOral Health 1-3&5Umar FarouqAinda não há avaliações
- PRE ANAESTHETIC ASSESSMENT New 1Documento41 páginasPRE ANAESTHETIC ASSESSMENT New 1lokeswara reddyAinda não há avaliações
- Location at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Documento5 páginasLocation at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Eduard RiparipAinda não há avaliações
- Multidisciplinary Ward Rounds Protocol at Arero HospitalDocumento6 páginasMultidisciplinary Ward Rounds Protocol at Arero Hospitalsami ketema100% (1)
- Guideline Antibiotic RationalDocumento35 páginasGuideline Antibiotic RationalIstianah EsAinda não há avaliações
- The Infection Control Manual: Standard PrecautionsDocumento5 páginasThe Infection Control Manual: Standard Precautionszenagit123456Ainda não há avaliações
- Health Management Information SystemDocumento6 páginasHealth Management Information SystemSSERWADDA ENOCK100% (1)
- Revised EMS Run SheetDocumento2 páginasRevised EMS Run Sheetanon-939227100% (2)
- Suctioning Techniques and ProceduresDocumento12 páginasSuctioning Techniques and ProceduresHannah Clarissa Faith AguilarAinda não há avaliações
- Medication ErrorDocumento3 páginasMedication Errortonlorenzcajipo100% (1)
- StrokeDocumento6 páginasStrokeRaulLopezJaimeAinda não há avaliações
- The Nurse in The Emergency Department Is Caring For A Patient With A PartialDocumento13 páginasThe Nurse in The Emergency Department Is Caring For A Patient With A Partialhasan ahmdAinda não há avaliações
- Blood Transfusions - TGH Policies & ProceduresDocumento4 páginasBlood Transfusions - TGH Policies & ProceduresMark Anthony FranciscoAinda não há avaliações
- Curriculum For NTA Level 5 Nursing PDFDocumento171 páginasCurriculum For NTA Level 5 Nursing PDFSOPHIA TWAHA0% (1)
- Nnp-Ii 2016-2020Documento88 páginasNnp-Ii 2016-2020Gebshet Woldetsadik100% (1)
- IV Therapy History and StandardsDocumento31 páginasIV Therapy History and Standardsrommelrn100% (1)
- Quality Indicators For ICU: Indian Society of Critical Care Medicine 2009Documento61 páginasQuality Indicators For ICU: Indian Society of Critical Care Medicine 2009akinravAinda não há avaliações
- HypertensionDocumento21 páginasHypertensionM RaisAinda não há avaliações
- International NursingDocumento18 páginasInternational NursingJennifer DixonAinda não há avaliações
- Nursing Leadership Roles ExplainedDocumento11 páginasNursing Leadership Roles ExplainedDimitri EroticoAinda não há avaliações
- 11.initial Assesment & Stabilization of Poly Trauma PatientsDocumento7 páginas11.initial Assesment & Stabilization of Poly Trauma PatientsmyscribeAinda não há avaliações
- Trends & Issues in MSN NursingDocumento41 páginasTrends & Issues in MSN NursingRajesh Sharma100% (3)
- Comprehensive Geriatric AssessmentDocumento7 páginasComprehensive Geriatric AssessmentJulien BulauanAinda não há avaliações
- Adult Assessment Tool 2014 (GOOD)Documento4 páginasAdult Assessment Tool 2014 (GOOD)Basinga Okinam100% (1)
- Pre-Embalming Observations: Arteries Injected: Veins Drained: Disinfection: (Check Appropriate Areas)Documento2 páginasPre-Embalming Observations: Arteries Injected: Veins Drained: Disinfection: (Check Appropriate Areas)May MontanoAinda não há avaliações
- Dell 1000W UPS Spec SheetDocumento1 páginaDell 1000W UPS Spec SheetbobAinda não há avaliações
- E2 PTAct 9 7 1 DirectionsDocumento4 páginasE2 PTAct 9 7 1 DirectionsEmzy SorianoAinda não há avaliações
- Case Study - Soren ChemicalDocumento3 páginasCase Study - Soren ChemicalSallySakhvadzeAinda não há avaliações
- 9780702072987-Book ChapterDocumento2 páginas9780702072987-Book ChaptervisiniAinda não há avaliações
- Continue: Adobe Project Voco DownloadDocumento3 páginasContinue: Adobe Project Voco DownloadLazlo SecretAinda não há avaliações
- Bar Exam 2016 Suggested Answers in Political LawDocumento15 páginasBar Exam 2016 Suggested Answers in Political LawYlnne Cahlion KiwalanAinda não há avaliações
- Khadi Natural Company ProfileDocumento18 páginasKhadi Natural Company ProfileKleiton FontesAinda não há avaliações
- BAM PPT 2011-09 Investor Day PDFDocumento171 páginasBAM PPT 2011-09 Investor Day PDFRocco HuangAinda não há avaliações
- Distribution of Laptop (Ha-Meem Textiles Zone)Documento3 páginasDistribution of Laptop (Ha-Meem Textiles Zone)Begum Nazmun Nahar Juthi MozumderAinda não há avaliações
- ADSLADSLADSLDocumento83 páginasADSLADSLADSLKrishnan Unni GAinda não há avaliações
- CORE Education Bags Rs. 120 Cr. Order From Gujarat Govt.Documento2 páginasCORE Education Bags Rs. 120 Cr. Order From Gujarat Govt.Sanjeev MansotraAinda não há avaliações
- 1LE1503-2AA43-4AA4 Datasheet enDocumento1 página1LE1503-2AA43-4AA4 Datasheet enAndrei LupuAinda não há avaliações
- Victor's Letter Identity V Wiki FandomDocumento1 páginaVictor's Letter Identity V Wiki FandomvickyAinda não há avaliações
- 6vortex 20166523361966663Documento4 páginas6vortex 20166523361966663Mieczysław MichalczewskiAinda não há avaliações
- Group 4-Hospital Information System - His - QuizDocumento2 páginasGroup 4-Hospital Information System - His - QuizGeeyan Marlchest B NavarroAinda não há avaliações
- Photoshop Tools and Toolbar OverviewDocumento11 páginasPhotoshop Tools and Toolbar OverviewMcheaven NojramAinda não há avaliações
- Server LogDocumento5 páginasServer LogVlad CiubotariuAinda não há avaliações
- (Free Scores - Com) - Stumpf Werner Drive Blues en Mi Pour La Guitare 40562 PDFDocumento2 páginas(Free Scores - Com) - Stumpf Werner Drive Blues en Mi Pour La Guitare 40562 PDFAntonio FresiAinda não há avaliações
- Unit 1 2marksDocumento5 páginasUnit 1 2marksLokesh SrmAinda não há avaliações
- Keya PandeyDocumento15 páginasKeya Pandeykeya pandeyAinda não há avaliações
- MSBI Installation GuideDocumento25 páginasMSBI Installation GuideAmit SharmaAinda não há avaliações
- Arizona Supreme CT Order Dismisses Special ActionDocumento3 páginasArizona Supreme CT Order Dismisses Special Actionpaul weichAinda não há avaliações
- Simplex Addressable Breakglass PDFDocumento12 páginasSimplex Addressable Breakglass PDFNurrul Ahmad Hidayat100% (1)