Você também pode gostar
- Microbiological Testing Technique of Pharmaceuticals Drugs1Documento74 páginasMicrobiological Testing Technique of Pharmaceuticals Drugs1Vinay Dhingra100% (1)
- DengueDocumento32 páginasDenguetummalapalli venkateswara rao100% (3)
- Dengue FeverDocumento8 páginasDengue FevervikasmaeAinda não há avaliações
- Dengue Biology ProjectDocumento14 páginasDengue Biology ProjectRohit Bhunia88% (8)
- DENGUEDocumento9 páginasDENGUERahul KhulbeyAinda não há avaliações
- Disinfectants in Pharmaceutical Industry Tim SandleDocumento8 páginasDisinfectants in Pharmaceutical Industry Tim SandleshwampaAinda não há avaliações
- Case Study DengueDocumento10 páginasCase Study DengueKathleen VargasAinda não há avaliações
- DengueDocumento9 páginasDengueWinna Gonato100% (2)
- Dengue Hemorrhagic FeverDocumento15 páginasDengue Hemorrhagic FeverAcca Malik MuhammadAinda não há avaliações
- TORCH in PregnancyDocumento63 páginasTORCH in PregnancyKinjal VasavaAinda não há avaliações
- Controlling Microbial Growth in Vivo Using Antimicrobial AgentsDocumento30 páginasControlling Microbial Growth in Vivo Using Antimicrobial AgentsJen PanganibanAinda não há avaliações
- Dengue Is Transmitted by The Bite of An Aedesmosquito Infected With Any One of The Four DengueDocumento6 páginasDengue Is Transmitted by The Bite of An Aedesmosquito Infected With Any One of The Four DengueKatrina PonceAinda não há avaliações
- DengueDocumento22 páginasDengueShekhar SinghAinda não há avaliações
- Pathophysiology: The Aedes MosquitoDocumento4 páginasPathophysiology: The Aedes MosquitoLlerym Onairda AzellebAinda não há avaliações
- World Mosquito DayDocumento18 páginasWorld Mosquito DayJennelyn TrinidadAinda não há avaliações
- Chapter 9 Dengue Fever 1Documento9 páginasChapter 9 Dengue Fever 1Kyla BalboaAinda não há avaliações
- Etiologic Agent: Fatality As High As 40-50%Documento7 páginasEtiologic Agent: Fatality As High As 40-50%Jolancr MarianoAinda não há avaliações
- To Study About DengueDocumento46 páginasTo Study About Denguekanha kumarAinda não há avaliações
- Dengue Fever: Dengue Fever (DF) Dengue Hemorrhagic Fever (DHF) Dengue Shock Syndrome (DSS)Documento4 páginasDengue Fever: Dengue Fever (DF) Dengue Hemorrhagic Fever (DHF) Dengue Shock Syndrome (DSS)Kirsten Kate SalesAinda não há avaliações
- IntroductionDocumento7 páginasIntroductionAdrian PunongbayanAinda não há avaliações
- Dengue Hemorrhagic FeverDocumento3 páginasDengue Hemorrhagic FeverhelimpAinda não há avaliações
- Prevention and Control Of: Dengue Hemorrhagic FeverDocumento19 páginasPrevention and Control Of: Dengue Hemorrhagic FeverClyde CapadnganAinda não há avaliações
- Dengue FeverDocumento17 páginasDengue FeverPuvanes GovindarajuAinda não há avaliações
- Dengue Hemorrhagic Fever Nursing Considerations and Nursing Care ManagementDocumento5 páginasDengue Hemorrhagic Fever Nursing Considerations and Nursing Care Managementjanns tumanengAinda não há avaliações
- DIREFDocumento6 páginasDIREFRahmongAinda não há avaliações
- Case Study DengueDocumento3 páginasCase Study Denguekevinramirez08Ainda não há avaliações
- Decee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverDocumento5 páginasDecee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverJeff Mac Rae RamosAinda não há avaliações
- Dengue 3y1 2Documento37 páginasDengue 3y1 2johnmichael008Ainda não há avaliações
- What Is Dengue FeverDocumento6 páginasWhat Is Dengue Feveroctober_7Ainda não há avaliações
- Dengue AwarenessDocumento4 páginasDengue AwarenesssatpalAinda não há avaliações
- Dengue MedscapeDocumento36 páginasDengue Medscapejeanne_mbAinda não há avaliações
- Dengue Hemorrhagic FeverDocumento3 páginasDengue Hemorrhagic FeverkewpietheresaAinda não há avaliações
- Transmission of Dengue FeverDocumento11 páginasTransmission of Dengue FeverPatricia E. Dela CruzAinda não há avaliações
- Dengue Syndrome: Presented By: A.Sahaya Mary M.SC Nursing I Yr Scon, SimatsDocumento57 páginasDengue Syndrome: Presented By: A.Sahaya Mary M.SC Nursing I Yr Scon, Simatssagi muAinda não há avaliações
- Journal Reading: Ade Cahyo Islami Dewinta Putri UtamiDocumento17 páginasJournal Reading: Ade Cahyo Islami Dewinta Putri UtamiAde Cahyo IslamiAinda não há avaliações
- Dengue Fever: Causes and SymptomsDocumento3 páginasDengue Fever: Causes and Symptomsteng SamsonAinda não há avaliações
- Dengue FeverDocumento4 páginasDengue FeverIjamSkemaAinda não há avaliações
- DengueDocumento9 páginasDengueGAIKWAD PREMAinda não há avaliações
- Case Study DengueDocumento10 páginasCase Study DengueKathleen VargasAinda não há avaliações
- Dengue FeverDocumento13 páginasDengue Feverjunathancortez123Ainda não há avaliações
- Local Media4912142242634097630Documento13 páginasLocal Media4912142242634097630Samantha Tiffany C. ManaloAinda não há avaliações
- DENGUEDocumento5 páginasDENGUEHpu JogindernagerAinda não há avaliações
- DENGUEDocumento31 páginasDENGUEVanlal RemruatiAinda não há avaliações
- Dengue Awarerness Program 2Documento19 páginasDengue Awarerness Program 2Ashok MaramAinda não há avaliações
- ND Dengue FeverDocumento6 páginasND Dengue FeverAlia SalviraAinda não há avaliações
- Biology Investigatory Projec Report Deng2Documento13 páginasBiology Investigatory Projec Report Deng2ghanshyamsamal2006Ainda não há avaliações
- Case Presentation 1Documento37 páginasCase Presentation 1Safoora RafeeqAinda não há avaliações
- Joel Vasanth PeterDocumento38 páginasJoel Vasanth PeterJoelPeterAinda não há avaliações
- What Is Dengue FeverDocumento5 páginasWhat Is Dengue FeverMuhammad Saad AhmadAinda não há avaliações
- Pathophysiology - Plasma Leakage Pathophysiology and Management of Dengue Hemorrhagic FeverDocumento1 páginaPathophysiology - Plasma Leakage Pathophysiology and Management of Dengue Hemorrhagic FeverKriz Mae Oñate DadaleAinda não há avaliações
- Dengue and Chikungunya Infections in ChildrenDocumento9 páginasDengue and Chikungunya Infections in ChildrenAl-Harits OctaAinda não há avaliações
- Dengue Fever: AssignmentDocumento9 páginasDengue Fever: AssignmentRohailAinda não há avaliações
- Dengue Fever Asignment 25.11.11Documento5 páginasDengue Fever Asignment 25.11.11jong188Ainda não há avaliações
- Dengue 121008123903 Phpapp02Documento34 páginasDengue 121008123903 Phpapp02maharshi mAinda não há avaliações
- Dengue Fever - 1Documento55 páginasDengue Fever - 1Anam AbidAinda não há avaliações
- Management of Dengue FeverDocumento13 páginasManagement of Dengue FeverGerald GarciaAinda não há avaliações
- Dengue FeverDocumento7 páginasDengue FeverTabarak BhuiyanAinda não há avaliações
- Communicable Diseases - ArticlesDocumento3 páginasCommunicable Diseases - ArticlesEzraManzanoAinda não há avaliações
- Dengue Fever Case StudyDocumento5 páginasDengue Fever Case StudyNadine PollescasAinda não há avaliações
- Dengue Fever - StatPearlsDocumento10 páginasDengue Fever - StatPearlskartini ciatawiAinda não há avaliações
- DBD English-1Documento7 páginasDBD English-1Risky Rahma Sari PutriAinda não há avaliações
- OpenMed 08 105 PDFDocumento11 páginasOpenMed 08 105 PDFMutia Diansafitri SuhudAinda não há avaliações
- Dengue FeverDocumento2 páginasDengue FeverIjaz SaddiquiAinda não há avaliações
- COVID19 Aanpak Van HVAC SystemenDocumento4 páginasCOVID19 Aanpak Van HVAC SystemenJan Willem van BorselenAinda não há avaliações
- Food IntoxicationDocumento34 páginasFood IntoxicationMuqtadir “The Ruler” KuchikiAinda não há avaliações
- Science of MicrobiologyDocumento11 páginasScience of MicrobiologyJamaica M DanguecanAinda não há avaliações
- Antimicrobial Activity From Leaf, Flower, Stem, and Root of Clitoria Ternatea - A ReviewDocumento6 páginasAntimicrobial Activity From Leaf, Flower, Stem, and Root of Clitoria Ternatea - A ReviewTung HuynhAinda não há avaliações
- The Plant Immune System: Jonathan D. G. Jones and Jeffery L. Dangl Nature, 2006Documento20 páginasThe Plant Immune System: Jonathan D. G. Jones and Jeffery L. Dangl Nature, 2006AnshulGuptaAinda não há avaliações
- Canine BabesiosisDocumento10 páginasCanine BabesiosisIonuț Gabriel ȚoleaAinda não há avaliações
- Ophthalmia NeonatorumDocumento5 páginasOphthalmia NeonatorumDelphy VargheseAinda não há avaliações
- Seminars in Diagnostic Pathology: Shawn R. Lockhart, Jeannette GuarnerDocumento5 páginasSeminars in Diagnostic Pathology: Shawn R. Lockhart, Jeannette GuarnerXXXI-JKhusnan Mustofa GufronAinda não há avaliações
- PneumoniaDocumento5 páginasPneumoniarjshubhAinda não há avaliações
- The Necessity of Evaluating The Effectiveness of Wearing The Face Shield With A Mask Only On The Mouth, As A Kind of Physical Precluding To Combat New Coronavirus OutbreakDocumento9 páginasThe Necessity of Evaluating The Effectiveness of Wearing The Face Shield With A Mask Only On The Mouth, As A Kind of Physical Precluding To Combat New Coronavirus OutbreakVIREMEDYAinda não há avaliações
- Specimen CollectionDocumento10 páginasSpecimen CollectionjaljimAinda não há avaliações
- Denagard Respiratory and Enteric Review (U. Klein)Documento8 páginasDenagard Respiratory and Enteric Review (U. Klein)nick224Ainda não há avaliações
- D3. Manual Book EngDocumento2 páginasD3. Manual Book EngMochamadSupriatnaAinda não há avaliações
- ICUD Urogenital InfectionsDocumento1.200 páginasICUD Urogenital InfectionsEladnemAinda não há avaliações
- West Nile Virus Fact SheetDocumento2 páginasWest Nile Virus Fact SheetWSETAinda não há avaliações
- (3)Documento20 páginas(3)Muhammad Hadi ArwaniAinda não há avaliações
- ObatDocumento1 páginaObatLiezna MusyarofaAinda não há avaliações
- Mycobacterium Abscessus For Drug DiscoveryDocumento11 páginasMycobacterium Abscessus For Drug DiscoveryShuaib AhmadAinda não há avaliações
- Giardia LambliaDocumento4 páginasGiardia LambliaUzziel Galinea TolosaAinda não há avaliações
- V21165607 Covid enDocumento2 páginasV21165607 Covid enMarjan JamshidiAinda não há avaliações
- Course Code Course Title Credit HRS.: Curriculum For Bs Biotechnology (4-Year Degree Programme)Documento48 páginasCourse Code Course Title Credit HRS.: Curriculum For Bs Biotechnology (4-Year Degree Programme)Momna AneesAinda não há avaliações
- Surgical Site Infection: Impacts and Challenges of Antibiotic RationalismDocumento8 páginasSurgical Site Infection: Impacts and Challenges of Antibiotic RationalismSabrina JonesAinda não há avaliações
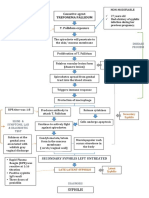
- Path o Physiology of SyphilisDocumento1 páginaPath o Physiology of Syphilis3S - JOCSON, DENESE NICOLE LEE M.Ainda não há avaliações
- Filariasis by Dr.T.V.Rao MDDocumento62 páginasFilariasis by Dr.T.V.Rao MDtummalapalli venkateswara raoAinda não há avaliações
- Laboratory Activity Revil Angelica MDocumento16 páginasLaboratory Activity Revil Angelica MAngelica Malacay RevilAinda não há avaliações
- Study Consent FormDocumento7 páginasStudy Consent FormMD YASIN BISWASAinda não há avaliações