Você também pode gostar
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Reason Prep's SAT Grammar Diagnostic Test AnalysisDocumento10 páginasReason Prep's SAT Grammar Diagnostic Test AnalysisMichelle Nugget UyAinda não há avaliações
- Review QuickBooks Online Assessment AnswersDocumento18 páginasReview QuickBooks Online Assessment AnswersYanah Flojo88% (8)
- SAT Math Formulas Cheat Sheet: The Ultimate GuideDocumento43 páginasSAT Math Formulas Cheat Sheet: The Ultimate GuideYanah Flojo100% (3)
- Section 1 - 5 QA DECOYDocumento18 páginasSection 1 - 5 QA DECOYYanah FlojoAinda não há avaliações
- Math ReviewerDocumento3 páginasMath ReviewerEunice Anne MitoAinda não há avaliações
- Compiled UPCAT Questions Language Reading - RtH7as PDFDocumento13 páginasCompiled UPCAT Questions Language Reading - RtH7as PDFJulius CagampangAinda não há avaliações
- Sat Vocab List V 2.1Documento21 páginasSat Vocab List V 2.1allmightymeetAinda não há avaliações
- Math ReviewerDocumento3 páginasMath ReviewerEunice Anne MitoAinda não há avaliações
- Compiled UPCAT Questions Mathematics - Dxgty9 PDFDocumento17 páginasCompiled UPCAT Questions Mathematics - Dxgty9 PDFMeg Angela Cirunay-DecenaAinda não há avaliações
- Starbucks Global Coffee GiantDocumento10 páginasStarbucks Global Coffee GiantYanah Flojo100% (1)
- Alternative HypothesisDocumento1 páginaAlternative HypothesisYanah FlojoAinda não há avaliações
- Module 1 Physics Basic ScienceDocumento23 páginasModule 1 Physics Basic SciencejudyaralarAinda não há avaliações
- Methods of DeliveryDocumento2 páginasMethods of DeliveryYanah FlojoAinda não há avaliações
- Evolution 1Documento1 páginaEvolution 1Yanah FlojoAinda não há avaliações
- StarbucksDocumento7 páginasStarbucksYanah FlojoAinda não há avaliações
- Courtship Traditions: Filipino Past vs PresentDocumento5 páginasCourtship Traditions: Filipino Past vs PresentYanah Flojo50% (8)
- Contemporary DevelopmentDocumento17 páginasContemporary DevelopmentMohammad AnisuzzamanAinda não há avaliações
- 6th Central Pay Commission Salary CalculatorDocumento15 páginas6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Higher Education Business & Management 2013Documento36 páginasHigher Education Business & Management 2013GerehAinda não há avaliações
- SHRMDocumento7 páginasSHRMpt_ngochauAinda não há avaliações
- Compentency-At A GlanceDocumento25 páginasCompentency-At A GlanceYanah FlojoAinda não há avaliações
- Higher Education Business & Management 2013Documento36 páginasHigher Education Business & Management 2013GerehAinda não há avaliações
- OsteomyelitisDocumento5 páginasOsteomyelitisYanah FlojoAinda não há avaliações
- HRM325 SuderlandDocumento536 páginasHRM325 SuderlandYanah Flojo100% (1)
- HRMDocumento58 páginasHRMYanah FlojoAinda não há avaliações
- NCP VMCDocumento6 páginasNCP VMCYanah FlojoAinda não há avaliações
- 15 16anaphysiofinalDocumento2 páginas15 16anaphysiofinalYanah FlojoAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Injuries To The Lumbosacral PlexusDocumento8 páginasInjuries To The Lumbosacral PlexusKhriz Ann C ÜAinda não há avaliações
- Auburn Trader - September 21, 2011Documento12 páginasAuburn Trader - September 21, 2011GCMediaAinda não há avaliações
- Lifern’s Anatomy: Limbs & TrunkDocumento161 páginasLifern’s Anatomy: Limbs & TrunkPauline MakahamadzeAinda não há avaliações
- Femoral Fracture Non-Union and Homoeoepathy - A Case ReportDocumento4 páginasFemoral Fracture Non-Union and Homoeoepathy - A Case ReportHomoeopathic Pulse100% (1)
- How To Read PalmsDocumento40 páginasHow To Read Palmsgur14100% (1)
- Understanding Child Abuse: Causes, Signs, SolutionsDocumento7 páginasUnderstanding Child Abuse: Causes, Signs, Solutionsdew23Ainda não há avaliações
- Roofing ActivitiesDocumento2 páginasRoofing ActivitiesArnold Roy Coballes Manalo100% (1)
- Walking Shoes: Features and Fit That Keep You Moving: by Mayo Clinic StaffDocumento3 páginasWalking Shoes: Features and Fit That Keep You Moving: by Mayo Clinic StaffRaprnaAinda não há avaliações
- Ian 167/12Documento23 páginasIan 167/12babarkhattakAinda não há avaliações
- Fit Fe: The Concept of Physical FitnessDocumento7 páginasFit Fe: The Concept of Physical FitnessJanna EchavezAinda não há avaliações
- Splint and TractionDocumento4 páginasSplint and TractionAMAZON PRIMEAinda não há avaliações
- Survival Manual TipsDocumento676 páginasSurvival Manual Tipssergey62100% (3)
- Chapter One (Ansci)Documento19 páginasChapter One (Ansci)Yumie YamazukiAinda não há avaliações
- Ankle Assessment AUT NotesDocumento32 páginasAnkle Assessment AUT Notesandimaree11Ainda não há avaliações
- Anatomy & Physiology TissuesDocumento13 páginasAnatomy & Physiology TissuesNicole Ken AgdanaAinda não há avaliações
- VIPower: VIPer22A Dual Output Reference Board 90 To 264 VAC Input, 10W OutputDocumento20 páginasVIPower: VIPer22A Dual Output Reference Board 90 To 264 VAC Input, 10W OutputLullaby summerAinda não há avaliações
- Murder Under Section 300Documento18 páginasMurder Under Section 300Yuvanesh KumarAinda não há avaliações
- Gujarat High Court Ordered Probe in Custodial Death Case - Shwetang Patel Murder Case - Patidar Agitation - Police Atrocity - (Read The Order)Documento9 páginasGujarat High Court Ordered Probe in Custodial Death Case - Shwetang Patel Murder Case - Patidar Agitation - Police Atrocity - (Read The Order)Manan BhattAinda não há avaliações
- Belt Failure AnalysisDocumento8 páginasBelt Failure AnalysisDavid ChandlerAinda não há avaliações
- Peripheral Nerve Lesions: Classification, Regeneration and Surgical StrategiesDocumento31 páginasPeripheral Nerve Lesions: Classification, Regeneration and Surgical StrategiesUjjawalShriwastavAinda não há avaliações
- Locked in SyndromeDocumento52 páginasLocked in SyndromeFarrukh Ali KhanAinda não há avaliações
- Modes of Mechanical VentilationDocumento4 páginasModes of Mechanical VentilationDuy ThanhAinda não há avaliações
- Special Test For All JointsDocumento42 páginasSpecial Test For All JointsVinothini Adaikkalasamy91% (45)
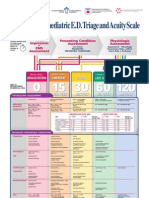
- Paediatric Triage PosterDocumento1 páginaPaediatric Triage PosterGenaro Olmos Garcia100% (2)
- Medical Report Template-88245311Documento29 páginasMedical Report Template-88245311Alvin WongAinda não há avaliações
- InvincibleDocumento10 páginasInvinciblesaz08100% (8)
- Dental Exam Questions on Conservative Dentistry and EndodonticsDocumento8 páginasDental Exam Questions on Conservative Dentistry and EndodonticsJude Aldo PaulAinda não há avaliações
- Penis Sonography. A Pictorial Review: Poster No.: Congress: Type: AuthorsDocumento35 páginasPenis Sonography. A Pictorial Review: Poster No.: Congress: Type: AuthorsOky Sutarto PutraAinda não há avaliações
- Treating Multiple Dental Injuries in a Teen Girl After a Car AccidentDocumento7 páginasTreating Multiple Dental Injuries in a Teen Girl After a Car AccidentDiego Andres Hincapie HerreraAinda não há avaliações
- Duchenne Muscular Dystrophy: An OverviewDocumento32 páginasDuchenne Muscular Dystrophy: An OverviewMr.P.Ramesh, Faculty of Physiotherapy, SRUAinda não há avaliações