Você também pode gostar
- Epidemiological Concepts for Causal InferencesDocumento4 páginasEpidemiological Concepts for Causal InferencesElizabeth100% (2)
- Epidemiology Practice Exam Answers FallDocumento20 páginasEpidemiology Practice Exam Answers Fallpmp123456Ainda não há avaliações
- Focused Antenatal CareDocumento49 páginasFocused Antenatal CareAbdullahi Kabir Suleiman100% (4)
- Quiz Public HealthDocumento26 páginasQuiz Public HealthMedShare89% (27)
- OHS Risk Management ProcedureDocumento9 páginasOHS Risk Management ProcedureBoroBethaMoneAinda não há avaliações
- Basic Concepts of EpidemiologyDocumento125 páginasBasic Concepts of EpidemiologyKailash Nagar100% (7)
- Unified Work Financial PlanDocumento9 páginasUnified Work Financial PlanMarieta Alejo0% (1)
- Question Bank EpidemiologyDocumento32 páginasQuestion Bank EpidemiologyRamesh Beniwal88% (8)
- Epidemiology MCQDocumento122 páginasEpidemiology MCQሌናፍ ኡሉም100% (1)
- Epidemiology Cheat SheetDocumento2 páginasEpidemiology Cheat SheetRichard Valdez100% (1)
- Historical Stages and Societal Influences on Community Health NursingDocumento30 páginasHistorical Stages and Societal Influences on Community Health NursingWithlove AnjiAinda não há avaliações
- EpidemiologyDocumento26 páginasEpidemiologymskotAinda não há avaliações
- Epidemiology Lecture NotesDocumento178 páginasEpidemiology Lecture NotesImtiaz Husain83% (6)
- Old MCQ EpidemiologyDocumento6 páginasOld MCQ EpidemiologyMartinc23100% (3)
- Epi Exam 2 Q&aDocumento13 páginasEpi Exam 2 Q&aeman100% (1)
- Case Control & Cross Sectional - Very HelpfulDocumento1 páginaCase Control & Cross Sectional - Very Helpfuldrnzyme89% (9)
- Community Health NursingDocumento7 páginasCommunity Health NursingFreeNursingNotes87% (47)
- Epidemiology MCQsDocumento4 páginasEpidemiology MCQsyooshlo78% (32)
- Epidemiology 2Documento54 páginasEpidemiology 2oheneapeahrita100% (2)
- Community Health NursingDocumento237 páginasCommunity Health Nursingjhing_apdan100% (2)
- Bnrs6222 Exam Answer Bnrs October 2020Documento6 páginasBnrs6222 Exam Answer Bnrs October 2020Cherry AdamsAinda não há avaliações
- Epidemiology MCQ 2Documento4 páginasEpidemiology MCQ 2Martinc2383% (12)
- Epidemiology MCQDocumento3 páginasEpidemiology MCQMartinc2350% (2)
- Practice Exercises For EpidemiologyDocumento8 páginasPractice Exercises For Epidemiologyninja-2001100% (2)
- Pediatric Nursing ReviewDocumento45 páginasPediatric Nursing Reviewɹǝʍdןnos98% (87)
- Observational Study DesignDocumento45 páginasObservational Study DesignIfanda Ibnu HidayatAinda não há avaliações
- Clerking An o & G CaseDocumento57 páginasClerking An o & G CaseAlan Na100% (2)
- EpidemiologyDocumento13 páginasEpidemiologyswethashaki50% (2)
- The Study of Disease Distribution and Determinants in PopulationsDocumento39 páginasThe Study of Disease Distribution and Determinants in PopulationsjayalakshmiAinda não há avaliações
- 1 Introduction To EpidemiologyDocumento39 páginas1 Introduction To EpidemiologySarahLiyana100% (1)
- Epidemiology QuestionsDocumento7 páginasEpidemiology Questionsbravof86% (7)
- Epidemiology ReviewDocumento29 páginasEpidemiology Reviewjohnkad100% (4)
- Epidemiology Measures and Formulas SimplifiedDocumento7 páginasEpidemiology Measures and Formulas SimplifiedAnonymous dNeWZoQ100% (3)
- Communicable Dse ReviewerDocumento13 páginasCommunicable Dse ReviewerRichard Ines Valino100% (29)
- Statistics in Public HealthDocumento20 páginasStatistics in Public HealthRiJade Bibiano100% (2)
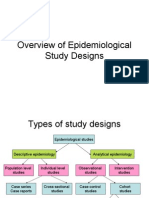
- Overview of Epidemiological Study DesignsDocumento16 páginasOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- Community Health Nursing Notes SummaryDocumento9 páginasCommunity Health Nursing Notes Summarysorryandreosayanisalreadytaken100% (28)
- Measuring Mortality and MorbidityDocumento13 páginasMeasuring Mortality and MorbidityIshika Roy100% (1)
- EpidemiologyDocumento101 páginasEpidemiologyeveeAinda não há avaliações
- Principles of Epidemiology in Public Health PracticeDocumento512 páginasPrinciples of Epidemiology in Public Health PracticeAdare Oluwafemi Thomas100% (3)
- Epidemiology NotesDocumento16 páginasEpidemiology NotesAnonymous 1I0JCC96G2100% (1)
- DR Nazia Sultan Ali B.D.S., M.P.H. Senior Demonstrator Fatima Jinnah Dental CollegeDocumento100 páginasDR Nazia Sultan Ali B.D.S., M.P.H. Senior Demonstrator Fatima Jinnah Dental Collegestpd2dogs100% (1)
- Epidermiology Unit 1Documento86 páginasEpidermiology Unit 1pushpa devkota100% (1)
- Community Health NursingDocumento8 páginasCommunity Health NursingFirenze Fil93% (30)
- Community Health Nursing ReviewerDocumento11 páginasCommunity Health Nursing Revieweroxidalaj88% (24)
- Final exam - infectious disease epidemiologyDocumento7 páginasFinal exam - infectious disease epidemiologyIsha Bhatt100% (1)
- Maternal & Child Care Nursing ReviewDocumento37 páginasMaternal & Child Care Nursing Reviewɹǝʍdןnos98% (130)
- Maternal & Child Care Nursing ReviewDocumento37 páginasMaternal & Child Care Nursing Reviewɹǝʍdןnos98% (130)
- Practice Quiz For EpidemiologyDocumento4 páginasPractice Quiz For EpidemiologyOsama Alhumisi100% (3)
- Epidemiology Review QuestionsDocumento12 páginasEpidemiology Review Questionsdrnzyme100% (6)
- Epidemiology: Andre Bencee V. Barimbao, RMT, MLS (ASCP)Documento55 páginasEpidemiology: Andre Bencee V. Barimbao, RMT, MLS (ASCP)Alondra Aran100% (2)
- MD3150E Epidemiology Biostatistics PDFDocumento10 páginasMD3150E Epidemiology Biostatistics PDFAhmad RajoubAinda não há avaliações
- Management of Tuberculosis: A guide for clinicians (eBook edition)No EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Ainda não há avaliações
- Managing Cleft Lip and Palate: An ENT PerspectiveDocumento27 páginasManaging Cleft Lip and Palate: An ENT PerspectiveAchmad HariyantoAinda não há avaliações
- Assignment 1 - YoungDocumento15 páginasAssignment 1 - Youngejyoung928100% (2)
- Basic EpidemiologyDocumento28 páginasBasic Epidemiologybijugeorge1100% (2)
- Answer of Exercises-Measures of Disease FrequencyDocumento7 páginasAnswer of Exercises-Measures of Disease Frequencysanjivdas100% (4)
- Epidemiology and Demography in Public HealthNo EverandEpidemiology and Demography in Public HealthJaphet KillewoNota: 5 de 5 estrelas5/5 (1)
- Community Health Nursing: I - Definition of TermsDocumento25 páginasCommunity Health Nursing: I - Definition of TermsRichard Ines Valino97% (29)
- Gapuz Notes Day 1-7Documento149 páginasGapuz Notes Day 1-7slapztikz91% (11)
- Analytical EpidemiologyDocumento64 páginasAnalytical EpidemiologyQueency Dangilan100% (1)
- EpidemiologyDocumento23 páginasEpidemiologyBabita DhruwAinda não há avaliações
- Epidemiologi Prof Bhisma MurtiDocumento32 páginasEpidemiologi Prof Bhisma MurtiniaasetaAinda não há avaliações
- Epidemiology Study Types and Designs ExplainedDocumento3 páginasEpidemiology Study Types and Designs Explainedbella.marie.cunningham6770100% (1)
- Veterinary Epidemiology (VEP-411)Documento15 páginasVeterinary Epidemiology (VEP-411)Vijay Kumar Anumolu100% (1)
- Cohort Study: Steps, Types, Advantages and ChallengesDocumento88 páginasCohort Study: Steps, Types, Advantages and Challengesankirana02Ainda não há avaliações
- Epidemiologic Study Designs: Dr. Sunita Dodani Assistant Professor Family Medicine, CHSDocumento23 páginasEpidemiologic Study Designs: Dr. Sunita Dodani Assistant Professor Family Medicine, CHSShubha DavalgiAinda não há avaliações
- EpidemiologyDocumento52 páginasEpidemiologyasdfsAinda não há avaliações
- Lesson 5 Epidemiology and Public Health For Med Students 2022-2023Documento62 páginasLesson 5 Epidemiology and Public Health For Med Students 2022-2023salemAinda não há avaliações
- Epidemiology in Community Health NursingDocumento25 páginasEpidemiology in Community Health NursingPornillosa, Jenaehl Mikhail S.Ainda não há avaliações
- What Is EpidemiologyDocumento34 páginasWhat Is EpidemiologyFYMAinda não há avaliações
- Premed - SPH - 2022Documento55 páginasPremed - SPH - 2022Tofik MohammedAinda não há avaliações
- Lec 2 Natural History of DiseaseDocumento23 páginasLec 2 Natural History of DiseaseAyesha ImtiazAinda não há avaliações
- EpidemiologyDocumento1 páginaEpidemiologySandeep KumarAinda não há avaliações
- Oral Epidemiology: Epidemiology. Dr. Mohamed Al-MontaserDocumento58 páginasOral Epidemiology: Epidemiology. Dr. Mohamed Al-Montaserغلاها عبدوAinda não há avaliações
- Distribution and Determinants of DiseaseDocumento6 páginasDistribution and Determinants of DiseaseNoreen FæţįmæAinda não há avaliações
- 2016 Unicef Stunting PSD - LKDocumento33 páginas2016 Unicef Stunting PSD - LKBheru LalAinda não há avaliações
- Public Health: Goal: To EnableDocumento12 páginasPublic Health: Goal: To EnableBheru LalAinda não há avaliações
- Physics For Nurses CON PIMSDocumento89 páginasPhysics For Nurses CON PIMSBheru Lal100% (1)
- Medication Errors: Mahmood AhmedDocumento10 páginasMedication Errors: Mahmood AhmedBheru LalAinda não há avaliações
- Community Health Nursing Notes Year One General Nursing in PakistanDocumento62 páginasCommunity Health Nursing Notes Year One General Nursing in PakistanBheru Lal100% (2)
- Maternal and Child Health in TheDocumento32 páginasMaternal and Child Health in TheBheru LalAinda não há avaliações
- Muscular DystrophyDocumento27 páginasMuscular DystrophyBheru LalAinda não há avaliações
- Anatomy and PhysiologyDocumento22 páginasAnatomy and PhysiologyBheru LalAinda não há avaliações
- Community Health Nursing Board ExamDocumento9 páginasCommunity Health Nursing Board ExamBheru LalAinda não há avaliações
- Characteristics of Clinical InstructorDocumento2 páginasCharacteristics of Clinical InstructorBheru LalAinda não há avaliações
- Nephrotic Syndrom Boook & NetDocumento10 páginasNephrotic Syndrom Boook & NetBheru LalAinda não há avaliações
- Job Description of Nursing ProfessionalsDocumento15 páginasJob Description of Nursing ProfessionalsBheru Lal100% (2)
- Cleft Lip & PalateDocumento24 páginasCleft Lip & PalateBheru Lal0% (1)
- Federal Public Service CommissionDocumento2 páginasFederal Public Service CommissionBheru LalAinda não há avaliações
- SociologyDocumento31 páginasSociologyBheru LalAinda não há avaliações
- Lecture NotesDocumento1 páginaLecture NotesBheru LalAinda não há avaliações
- CV Allen Alcantara EditedDocumento3 páginasCV Allen Alcantara EditedAlcntara AllenAinda não há avaliações
- WM-1249-EN-001 PrenaTest Key Paper Summary PMCF-StudyDocumento2 páginasWM-1249-EN-001 PrenaTest Key Paper Summary PMCF-StudytcAinda não há avaliações
- Emergency Contraception Use Among Undergraduate Students of The University of Professional Studies - July 2016Documento89 páginasEmergency Contraception Use Among Undergraduate Students of The University of Professional Studies - July 2016fzguokeAinda não há avaliações
- Role of NGOs in AIDS Control Programme DR Joseph P CarelDocumento115 páginasRole of NGOs in AIDS Control Programme DR Joseph P CarelCarel Joseph0% (1)
- Klebsiella Pneumoniae TreatmentDocumento2 páginasKlebsiella Pneumoniae Treatmentil_memoAinda não há avaliações
- Pregnancy Nausea and Vomiting GuideDocumento16 páginasPregnancy Nausea and Vomiting Guidezakariah kamalAinda não há avaliações
- PPP's Vision for an Inclusive Ghanaian SocietyDocumento24 páginasPPP's Vision for an Inclusive Ghanaian SocietyMartin SekyiAinda não há avaliações
- Cais25 PDFDocumento4 páginasCais25 PDFSpreading KnowledgeAinda não há avaliações
- Intermittent Fasting: By: Avital SchwartzDocumento2 páginasIntermittent Fasting: By: Avital SchwartzMossa SultanyAinda não há avaliações
- Halaman Judul SkripsiDocumento18 páginasHalaman Judul SkripsiAgnes NababanAinda não há avaliações
- Milroy Disease Pak TomoDocumento3 páginasMilroy Disease Pak TomoMeta SariAinda não há avaliações
- Important Estimates in Pregnancy & Danger Signs in Pregnancy PDFDocumento3 páginasImportant Estimates in Pregnancy & Danger Signs in Pregnancy PDFTandingco, Olivia Mari H.Ainda não há avaliações
- (15th June - 21st June) Weekly Webinars ScheduleDocumento1 página(15th June - 21st June) Weekly Webinars ScheduleSahil DhamijaAinda não há avaliações
- Evaluating Diagnostics: A Guide For Diagnostic EvaluationsDocumento5 páginasEvaluating Diagnostics: A Guide For Diagnostic EvaluationsYanneLewerissaAinda não há avaliações
- Wastewater Treatment and RecyclingDocumento8 páginasWastewater Treatment and RecyclingSudheer NaniAinda não há avaliações
- Postpartal Pueperal InfectionDocumento38 páginasPostpartal Pueperal InfectionIrish Jane Bayle CubilloAinda não há avaliações
- Lines of Inquiry Brinly Meelia 1Documento5 páginasLines of Inquiry Brinly Meelia 1api-710190426Ainda não há avaliações
- Quick Start Oral ContraceptivesDocumento2 páginasQuick Start Oral ContraceptivesAnna DangAinda não há avaliações
- Edukasi Perilaku Hidup Sehat Dan Bersih Sebagai Upaya Pencegahan Penularan Virus Covid-19Documento18 páginasEdukasi Perilaku Hidup Sehat Dan Bersih Sebagai Upaya Pencegahan Penularan Virus Covid-19Kriz AdinataAinda não há avaliações
- BGD Health System Review PDFDocumento214 páginasBGD Health System Review PDFSawbanAinda não há avaliações
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Documento2 páginasIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)ShakirShafiAinda não há avaliações
- Pneumonia Lobaris PneumoniaDocumento34 páginasPneumonia Lobaris PneumoniamoditiaraAinda não há avaliações
- SML Safety ShortDocumento17 páginasSML Safety Shortzale barunaAinda não há avaliações
- Gestational DiabetesDocumento42 páginasGestational Diabetesjohn jumborock100% (1)
- Covid-19 Mass Vaccination PlanDocumento95 páginasCovid-19 Mass Vaccination PlanJeremy Turley100% (1)
- Pharmacovigilance 1Documento28 páginasPharmacovigilance 1Gideon AdurojaAinda não há avaliações