Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- ServSafe 7th Edition Full PDFDocumento366 páginasServSafe 7th Edition Full PDFAissie Tribiana90% (49)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- RISK MANAGEMENT (Midterm & Final) PDFDocumento25 páginasRISK MANAGEMENT (Midterm & Final) PDFJas John75% (4)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Alternatives For Allergens in The 2018 American.2-1 PDFDocumento19 páginasAlternatives For Allergens in The 2018 American.2-1 PDFamila yashifaAinda não há avaliações
- Module 5 TranscriptDocumento27 páginasModule 5 TranscriptHakim AliAinda não há avaliações
- G CP CompiledDocumento120 páginasG CP CompiledMelody Kaye MonsantoAinda não há avaliações
- Acknowledgement, Intro, Profile, Directory, Economic ProposalDocumento34 páginasAcknowledgement, Intro, Profile, Directory, Economic ProposalMelody Kaye MonsantoAinda não há avaliações
- Super Final Output (For Hardbound)Documento108 páginasSuper Final Output (For Hardbound)Melody Kaye MonsantoAinda não há avaliações
- Acute Pain..Documento2 páginasAcute Pain..Melody Kaye MonsantoAinda não há avaliações
- "Change" (A Synthesis Paper) in Partial Fulfillment of The Requirements in FFPDocumento4 páginas"Change" (A Synthesis Paper) in Partial Fulfillment of The Requirements in FFPMelody Kaye MonsantoAinda não há avaliações
- Acute Pain..Documento2 páginasAcute Pain..Melody Kaye MonsantoAinda não há avaliações
- A Moment Like This LyricsDocumento2 páginasA Moment Like This LyricsMelody Kaye MonsantoAinda não há avaliações
- Invitation OutlineDocumento1 páginaInvitation OutlineMelody Kaye MonsantoAinda não há avaliações
- Name Ambreen Fazal Roll No MS-HND-17-05 Submitted To Sir Tariq IsmailDocumento16 páginasName Ambreen Fazal Roll No MS-HND-17-05 Submitted To Sir Tariq IsmailHAMMAD FAZALAinda não há avaliações
- Rinitis AlergicaDocumento6 páginasRinitis Alergicaismael_132Ainda não há avaliações
- Review of Literature - Anusha BhandarkarDocumento26 páginasReview of Literature - Anusha BhandarkarAnushaAinda não há avaliações
- Foreign Body Reactions, Marginal Bone Loss and Allergies in Relation To Titanium Implants AlbrektssonDocumento11 páginasForeign Body Reactions, Marginal Bone Loss and Allergies in Relation To Titanium Implants AlbrektssonImplantologia Oral y ReconstructivaAinda não há avaliações
- Food AllergensDocumento13 páginasFood AllergenskrishnamythriAinda não há avaliações
- (Pulmo) 2020 AriaDocumento29 páginas(Pulmo) 2020 AriaerikaAinda não há avaliações
- Daily Express 2011.04.22Documento80 páginasDaily Express 2011.04.22Ник ЧенAinda não há avaliações
- Theunis, Louise Immunotherapeutics CapstoneDocumento4 páginasTheunis, Louise Immunotherapeutics CapstoneLouise TheunisAinda não há avaliações
- Allergic Disease: Prof. Rusudan Karseladze Iv. Javakhishvili Tbilisi State University Institute of PediatricsDocumento144 páginasAllergic Disease: Prof. Rusudan Karseladze Iv. Javakhishvili Tbilisi State University Institute of PediatricspalAinda não há avaliações
- The Allergy Book - Solving Your Family's Nasal Allergies, Asthma, Food Sensitivities, and Related Health and Behavioral Problems (PDFDrive)Documento282 páginasThe Allergy Book - Solving Your Family's Nasal Allergies, Asthma, Food Sensitivities, and Related Health and Behavioral Problems (PDFDrive)angelobuffaloAinda não há avaliações
- Nanoe Tech Panasonic PDFDocumento10 páginasNanoe Tech Panasonic PDFRoland MichaelAinda não há avaliações
- Allergic Rhinitis & Vasomotor Rhinitis: Dr. Ritesh Mahajan ENT Consultant GMC, KathuaDocumento70 páginasAllergic Rhinitis & Vasomotor Rhinitis: Dr. Ritesh Mahajan ENT Consultant GMC, Kathuamanoj kumarAinda não há avaliações
- Food AllergensDocumento20 páginasFood Allergenssyed zia ul hassanAinda não há avaliações
- DR Darin Ingels - 7-28-10Documento37 páginasDR Darin Ingels - 7-28-10NAA NYC Metro ChapterAinda não há avaliações
- Nature's Pathways April 2014 Issue - Northeast WI EditionDocumento96 páginasNature's Pathways April 2014 Issue - Northeast WI EditionNature's PathwaysAinda não há avaliações
- Anaphylactic ShockDocumento36 páginasAnaphylactic ShockCarmelli Mariae Calugay100% (1)
- Patch TestingDocumento1 páginaPatch Testing26 ThufailAinda não há avaliações
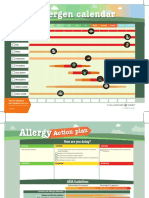
- Allergen Calendar - EnglishDocumento2 páginasAllergen Calendar - Englishpkgill15Ainda não há avaliações
- Allergic Reactions in EndodonticDocumento8 páginasAllergic Reactions in EndodonticDr.O.R.GANESAMURTHIAinda não há avaliações
- Ephedra FoliataDocumento16 páginasEphedra Foliatavishwanathz47Ainda não há avaliações
- Upper Airway DisordersDocumento25 páginasUpper Airway DisordersIliana EsquivelAinda não há avaliações
- Manufacture of NR GloveDocumento12 páginasManufacture of NR Glovesimbua72Ainda não há avaliações
- Flu Letter To Parents 2015 - BVE - EditsDocumento2 páginasFlu Letter To Parents 2015 - BVE - EditsSusan Loida SorianoAinda não há avaliações
- Health 6 w7 Explain The Effect of Pests and Rodents To One's HealthDocumento73 páginasHealth 6 w7 Explain The Effect of Pests and Rodents To One's HealthDell Sabugo CorderoAinda não há avaliações
- Harvard Medical School Controlling Your AllergiesDocumento57 páginasHarvard Medical School Controlling Your Allergiesjennieval100% (1)
- Product Sheet ImmunoCAP Rapid Wheeze Rhinitis ChildDocumento2 páginasProduct Sheet ImmunoCAP Rapid Wheeze Rhinitis ChildYuriiAinda não há avaliações