Vaccine 22 (2003) 287292
Long-term persistence of immunity after immunisation with Haemophilus inuenzae type b conjugate vaccine
P. Helena Mkel a , Helena Kyhty a, , Tuija Leino a , Kari Auranen a,b , Heikki Peltola c , Nina Ekstrm a , Juhani Eskola a,1
c a National Public Health Institute, Mannerheimintie 166, FIN-00300 Helsinki, Finland Rolf Nevanlinna Institute, University of Helsinki, PL 4, 00014 Helsingin yliopisto, Finland Hospital for Children and Adolescents, University of Helsinki, PL 281, 00029HUS Helsinki, Finland b
Received 2 January 2002; received in revised form 10 May 2002
Abstract Although Haemophilus inuenzae type b (Hib) conjugate vaccines, after licensure in 1987, are now recommended for world-wide use, the duration of protective immunity afforded by them is not known. We therefore assessed the immunogenity at 910 years of age in 37 children who had received the rst Hib conjugate, PRP-D, in infancy (the Hib-conjugate group) and were now given a dose of Hib polysaccharide (PS) as a test vaccine. The anti-Hib PS antibodies (Hib-ab) were measured before and after this test vaccination, and the values compared to those in 37 control children who had not previously received any Hib vaccine and in 13 children who had received Hib PS vaccine in infancy (the Hib-PS group). Prior to the test vaccination, the Hib-ab concentrations in the Hib-conjugate group were 3.6-fold higher than in the control group. After the test vaccination, the Hib-conjugate group had higher total Hib-ab concentrations, higher proportion of IgG and higher avidity of Hib-ab than the control or the Hib-PS group, suggesting persisting immunological memory in a Hib-c group. A mathematical model, including memory, predicted accurately the Hib-ab concentrations, which are maintained through anamnestic responses to intervening stimuli (Hib or cross-reacting bacteria). 2003 Published by Elsevier Ltd.
Keywords: Haemophilus inuenzae type b; Duration of immunity; Modelling
1. Introduction Conjugate vaccines, in which the immunising potential of bacterial cell surface polysaccharides (PS) has been enhanced by covalent coupling to protein, are important new tools in prevention of infectious diseases. The rst such vaccine, the Haemophilus inuenzae type b (Hib) conjugate vaccine has resulted in virtual elimination of invasive Hib disease in the countries that have included it in their infant immunisation programs [14]. A large amount of knowledge of the special features associated with the novel vaccine type, combining properties of polysaccharide and protein antigens, has been obtained through the Hib model, i.e. clinical trials and subsequent large-scale use of the vaccine. Recently, two further conjugate vaccines have been licensed. Together, these vaccines against the three foremost
Corresponding author. Tel.: +358-9-47441; fax: +358-9-47448599. E-mail address: helena.kayhty@ktl. (H. Kyhty). 1 Present address: Aventis Pasteur, 2 avenue Pont Pasteur, F69367 Lyon Cedex 07, France. 0264-410X/$ see front matter 2003 Published by Elsevier Ltd. doi:10.1016/S0264-410X(03)00524-3
bacterial causes of acute respiratory infections and meningitis, Hib, Streptococcus pneumoniae and Neisseria meningitidis, could have a major impact on the disease burden in both developing and industrial countries. A thorough understanding of the rules and limitations of protective immunity elicited by the conjugate vaccines would be important in preparation for their extensive worldwide use. In the present article, we address a key question, i.e. the duration of immunity and the consequent need of revaccination in the Hib model. In the unvaccinated population serum antibodies to Hib PS develop from approximately 2 years of age on in response to subclinical infections (carriage) by Hib and other bacteria that have cross-reacting PS structures [58]. A plateau of approximately 12 g/ml is sustained through adulthood [1], presumably in response to similar random encounters with the Hib antigen. In this setting, the antibody concentration predicting protection was identied as 0.15 g/ml [1,9,10] and a mathematical model constructed to predict antibody persistence after an initial response to Hib PS [11,12].
288
P.H. Mkel et al. / Vaccine 22 (2003) 287292
The response to the conjugate vaccine differs from the above-described response to Hib PS in three aspects: an antibody response is obtained earlier, the response is higher, and the responses to later antigenic stimuli are likely to be both higher and more rapid anamnestic responses because of the immunological memory elicited [1316]. To learn how these features, and especially the immunological memory affect the duration of immunity we studied 910-year-old children who had participated 8 years earlier in immunogenicity studies with Hib conjugate (Hib-c) or PS vaccines. Their anti-Hib concentration was compared to the concentration in control children who had never received Hib vaccine. Then the three groups of children were given a dose of Hib PS as a test vaccine for immunological memory and their responses assessed for antibody quantity, isotype and avidity. Furthermore, the mathematical model of antibody persistence after Hib PS immunisation was modied to take into account the special features associated with conjugate vaccines. 2. Materials and methods 2.1. Subjects All children were recruited to the study during 19931994 at the Health Centre of Joensuu, Finland. The study protocol was approved by the Ethics Committee of the National Public Health Institute, Helsinki, Finland. 2.1.1. The Hib conjugate vaccine group Thirty-seven children (mean age 9.5 years, range 9.010.5) had participated in early immunogenicity studies [16,17] in the same location and received the Hib conjugate vaccine PRP-D (Connaught Laboratories Inc., Swiftwater, PA) as four injections between the ages of 3 and 18 months. 2.1.2. The control group Thirty-nine children (mean age on recruitment 9.8, range 9.010.6) had not received any Hib vaccine previously. 2.1.3. The Hib-PS vaccine group Thirteen children from a previous study [16], who had received Hib-PS vaccine (10 g of Hib PS per dose, lot 7-1391-002; Lederle Laboratories, Pearl River, NY or 25 g of Hib PS per dose, lot 3799, Connaught Laboratories Inc.) as four injections between the ages of 3 and 18 months were recruited to this study at the mean age of 10.4 years (range 10.310.6 years). 2.2. Samples and test vaccination with Hib PS A venous blood sample was drawn from all children on recruitment. After this the children were vaccinated with the Hib PS vaccine PRP (25 g/0.5 ml). The vaccine (lot B) was prepared by Wyeth Lederle Paediatrics and Vaccines, Rochester, NY, described under FDA PLA no 83-362 and
received from Dr. Pamela McInnes, Food and Drug Administration, Bethesda, MD. No other vaccines were given at the same time. A second blood sample was drawn 4 weeks later. The serum was separated and stored in aliquots at 20 C until use. 2.3. Antibody assays and previous data Total anti-Hib PS antibody concentrations were determined by radioimmunoassay (RIA) [18]. The same assay and the same reference serum (lot 1983) received from Centre for Biological Evaluation & Research (CBER), Bethesda, MD, that contained 70 g/ml of anti-Hib PS has been used when the antibody response to the primary immunisations was determined. Furthermore, the same in house control sera were used throughout the present and the previous studies. From those children that had received Hib vaccines in early childhood, we had antibody data from samples taken up to 2 years of age [16,17], unpublished. In addition, we had antibody data from our previous studies of unimmunised children at the same ages [1619]. Immunoglobulin class specic antibody concentrations were determined by enzyme immunoassay (EIA) as described [16] with minor modications using Hib oligosaccharides conjugated to human serum albumin (HbOHA) [20] received from Porter Anderson (University of Rochester, Rochester, NY) as coating antigen. The two-tailed Students t-test was used to test the signicance of differences between antibody concentrations in different study groups. Avidity of anti-Hib PS antibodies was measured as described by Goldblatt et al. [21] with a modication described by Anttila et al. [22]. In short, wells of polystyrene plates (Costar, Cambridge, MA) were coated with HbOHA [20]. Low avidity antibodies were detached by 0.2 M sodium thiocyanate and the percentage of antibody left after this treatment was calculated as relative avidity index. 2.4. Mathematical model We formulated a model for the decline of anti-Hib PS antibody concentrations after Hib-c vaccination that took into account the initial response, the subsequent decay of concentration, and the possible restimulation due to encounters with Hib or cross-reacting bacteria. The model for a polysaccharide-type response to vaccine and natural antigenic stimuli has been described by Auranen et al. [11]. The implications of this model have been further investigated by Leino et al. [12]. In the present study, we modied the two key parameters. First, the response to vaccine (now response to the fourth dose of Hib conjugate vaccine) was estimated from observed responses to Hib conjugate vaccine at 1.5 years of age (N = 113, estimated mean response 45 g/ml, 95% of responses within interval 4508 g/ml, unpublished data). Second, the same log-normal distribution was assumed to characterise the anamnestic, memory type responses to subsequent antigenic stimuli. These stimuli
P.H. Mkel et al. / Vaccine 22 (2003) 287292
289
were taken to occur at a rate of 0.25 per year at random encounters with Hib or cross-reacting bacteria [11].
Anti-Hib at 9 to 10 yr, ug/ml
100
10
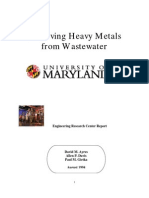
3. Results The life history of anti-Hib antibodies in the serum of the 37 Hib conjugate vaccine recipients (Hib-c group) (Fig. 1) shows the transplacentally acquired antibodies rapidly declining in the rst months of life, the response to the primary series of three Hib-c injections given between 3 and 7 months, the subsequent decline to the age of 1.5 years, followed by a strong response to the booster dose of vaccine, and again a decline in the next 6 months. All this corresponds to previously described responses to Hib conjugate vaccines. The new data show that in the subsequent years, up to 8 years from the last vaccine dose, there was negligible further decrease of the mean serum anti-Hib concentration, which thus remained at 3.4 g/ml. The gure also shows the development of natural immunity to Hib in the control group of children who had never received Hib vaccine (an increase of the mean anti-Hib concentration from 0.16 g/ml at 2 years to 0.94 g/ml at 910 years). Thus, the Hib conjugate vaccine recipients had at 910 years of age 3.6-fold more (P < 0.001) antibodies to Hib PS than the control group. The antibody was mainly IgG in both groups, and the mean avidity index 51.1 in the Hib-c group and 45.9 in the control group (Table 1). The antibody concentrations at 910 years of age in the 37 Hib-c group children varied widely from 0.1 to 100 g/ml as shown by Fig. 2 in which they are plotted against the antibody levels of the same children at 2 years of age. Of
0.1
0.01 0.01 0.1 1 10 100 1000
Anti-Hib at 24 or 36 mo, ug/ml
Fig. 2. Comparison of concentrations ( g/ml) of anti-Hib PS at the age of 2 years (X-axis) and at 910 years (Y-axis) in sera of children immunised with four doses of Hib conjugate vaccine PRP-D between the ages of 3 and 18 months. Children with >4-fold higher concentration at 910 years than at 2 years are indicated with an open square.
note is that in six children the antibody concentrations at 910 years were 310 times higher than at 2 years, strongly suggesting an intervening antigenic stimulus. However, as the stimuli themselves were not observed it was not possible to tell from these data whether or not the response was an anamnestic response indicative of memory. To this end, we used a different approach, i.e. giving a test dose of Hib PS to the Hib-c group of children and comparing their responses to the responses in the control group of children who had not received a Hib vaccine before. The ndings were consistent with immunologic memory in the
100
10 Anti-Hib, ug/ml
0.1
0.01 0 1 2 3 4 5 Age, years
Fig. 1. The development from birth to 10 years of serum antibodies to Hib PS in children who have received four doses of the Hib conjugate vaccine PRP-D between 3 and 18 months of age (solid line) or no Hib vaccine (dotted line), based on data from the authors laboratory ([1619], present study, unpublished).
10
290
P.H. Mkel et al. / Vaccine 22 (2003) 287292
Table 1 Serum antibodies to Haemophilus inuenzae type b (Hib) polysaccharide (PS) in 910 years old children before or 1 month after a test dose of Hib PS vaccine Before test dose of Hib PS No Hib Anti-Hib PS (N) IgG IgM IgA Relative avidity (N)d Avidity index 39 0.63 (0.460.87) 0.15 (0.130.17) 0.13 (0.120.15) 27 45.9 (37.953.9) Hib-c 37 5.76a (4.697.08) 0.16 (0.150.18) 0.19 (0.150.23) 34 51.1 (44.657.5) After test dose of Hib PS No Hib 39 28.6 (23.335.0) 1.57 (1.231.99) 3.02 (2.393.81) 27 41.2 (34.148.3) Hib-c 36 107.7a (88.2131.4) 0.60b (0.500.72) 4.35 (3.515.40) 34 50.5c (45.156.0)
The children had either never received Hib vaccine (No Hib) or received (Hib-c) the Hib conjugate vaccine PRP-D as four doses between the ages of 3 and 18 months. The antibody concentrations ( g/ml) were measured by enzyme immunoassay (EIA) and given as the mean (95% CI). The relative avidity of the IgG was measured by thiocyanate EIA and is given as the avidity index. a <0.001; Hib-c > no Hib. b <0.01; Hib-c < no Hib. c <0.05; Hib-c > no Hib. d Relative avidity assay required an anti-Hib IgG concentration of 0.1 g/ml hence not all sera could be assayed.
Hib-c group: a higher mean total post-vaccination anti-Hib PS antibody concentration (77.8 compared to 39.1 in the control group, P < 0.01), and a higher mean IgG class anti-Hib PS concentration (P < 0.001, Table 1). The mean IgM concentration was lower (P < 0.01) and the mean IgA concentration the same in the Hib-c group as compared to the control group. Furthermore, the avidity index was significantly higher in the Hib-c group (50.5) than in the control group (41.2, P < 0.05, Table 1). A further control group consisted of children who had in our earlier studies received the Hib PS vaccine with the same schedule as used for Hib-c [16]. Thirteen of these children were available for the present study at 910 years of age. At this time, their mean anti-Hib PS concentration was
0.75 g/ml, not signicantly different from that of previously non-vaccinated children (0.94 g/ml). Their antibody response to the test vaccination with Hib PS at this time was also not different in quantity (mean, 48.2 g/ml) or Ig class distribution (GMCs of 40.9, 1.3 and 3.2 g/ml of IgG, IgM and IgA, respectively) from the children who had previously not received any Hib vaccine. To have a general model for predicting antibody persistence from data on antibody concentrations after Hib-c vaccination we modied the mathematical model previously developed for Hib PS vaccination to include the higher, anamnestic response to intervening stimuli. Fig. 3 shows the predicted distribution of the anti-Hib GMC in our Hib-c study group at 10 years of age under the Hib-PS
Fig. 3. Predictive distribution of the geometric mean anti-Hib PS antibody concentration ( g/ml) at 10 years of age in a cohort of 37 children who have received their fourth dose of Hib conjugate vaccine PRP-D at 1.5 years of age. The actual observed value 3.4 g/ml is marked by an arrowhead. Distributions are presented for the model developed for Hib PS vaccine (panel A), and for the modied model including memory after the Hib conjugate vaccine (panel B).
P.H. Mkel et al. / Vaccine 22 (2003) 287292
291
response-based model (panel A), and the modied, anamnestic response-based model (panel B). It is evident that the PS model gave too low predicted values in comparison to the observed GMC (3.4 g/ml; marked by arrowhead) whereas the t under the conjugate model in panel B was excellent.
4. Discussion We found that the anti-Hib concentrations in 910 years old children 8 years after Hib conjugate vaccination were 3.6-fold greater than in children who had never received Hib vaccine. The persistence of the anti-Hib concentrations was much longer than after vaccination with Hib PS vaccine; the 13 children who had received Hib PS in infancy that we could trace 8 years later had antibody concentrations not differing from the GMC in previously unvaccinated children. This nding supports previous data from a 4.5-year follow-up study in Sweden [23] and 3-year follow-up studies in UK and Canada [24,25]. The antibody concentrations reported in the Swedish study (2.1 g/ml) at 6 years, and in Canada (2.2 g/ml) at 45 years are rather close to the 3.4 g/ml found in this study at 10 years of age although the conjugate vaccines used differed (PRP-T in Sweden and Canada, the generally less immunogenic PRP-D in Finland [19]). In our study and the study from Canada with the very satisfactory long-term results, the conjugate was given as three doses in infancy, followed by a booster dose in the second year of life. By contrast, in Sweden only three doses of PRP-T between 3 and 12 months gave a good result [23]. Less satisfactory results have been seen 23 years after one dose of PRP-D given at 19 months of age in Canada (GMC 0.7 g/ml [25]), after four doses of PRP-T in The Netherlands (GMC 0.8 g/ml [26]) and 3 and 4 years after the same vaccine given in the UK program at 2, 3, and 4 months of age (1.06 and 0.89 g/ml, respectively [24]). Whether the different schedules will sufce to provide sustained protection from disease and carriage in the long run remains to be seen. We also found long-term persistence of a high, IgG dominated response to Hib PS vaccine in the recipients of the Hib conjugate vaccine compared to children who previously had received only Hib PS or no Hib vaccine. A similar test for persistence of memory has been reported from the UK 3 years after vaccination with PRP-T at 2, 3 and 4 months of age [24]. The higher relative avidity of IgG antibody evoked in the present study by the Hib PS 8 years after vaccination with the conjugate vaccine further supports the concept of an anamnestic response and long persistence of memory. In the present study, we furthermore showed that the response to intervening unobserved stimuli is an essential element in the persistence of elevated serum antibody concentrations after Hib conjugate vaccinessee examples in Fig. 2. Mathematical modelling has provided additional evidence of the role of restimulation in persistence of anti-Hib
PS antibodies [11,12]. The model was initially developed for antibodies stimulated by Hib PS vaccine, but was modied in the present study to accommodate stronger anamnestic responses to intervening stimuli during the 8 years follow up after Hib-c vaccination. A comparison of the predicted antibody concentrations at 10 years of age with the observed value showed that this modication was essential. An uncertainty in these calculations was the value of the force of infection, i.e. the rate of encounters with antigenic stimuli previously estimated as 0.25 per year [27]. On one hand, this level might be an over-estimate for the present study as the prevalence of Hib carriage in the study population may have decreased due to herd immunity generated by the introduction of Hib-c vaccine in Finland during the 8 years follow-up time of this study [2]. On the other hand, there is no evidence suggesting that the frequency of stimuli due to the cross-reactive bacteria would have decreased. In fact, the observed anti-Hib concentrations (0.94 g/ml) in the 910-year-old children in this study who had not received Hib vaccine was similar to adult levels before the conjugate immunisation era, strongly arguing for continued antigenic stimuli in the population. In conclusion, we have shown that immunity to Hib can persist for at least 8 years after vaccination with Hib conjugate vaccine in infancy. The persistence depends on repeated antigenic stimuli provided by both Hib and cross-reacting bacteria, and the strong anamnestic responses to these stimuli due to long-lasting immunologic memory. The same elements are likely to play a role in persistence of immunity elicited by both pneumococcal and meningococcal vaccines. It would therefore be wise to collect data on their magnitude as a basis of a rational design of future vaccination programs.
Acknowledgements We thank Teija Jaakkola and Sirkka-Liisa Wahlman for technical assistance in the antibody assays, Pirjo-Riitta Saranp and Minna Huittinen for recruiting, taking blood samples and vaccinating the children. Dr. Pamela McInnes (NIH, Bethesda, MD) provided the Hib vaccine for the study.
References
[1] Mkel P, Eskola J, Kyhty H, Takala A. Vaccines against Haemophilus inuenzae type b. In: Ala Aldeen DAA, Hormaeche CE, editors. Molecular and Clinical Aspects of Bacterial Vaccine development. Wiley, Chichester; 1995. p. 4191. [2] Eskola J, Kyhty H. Ten years experience with Hib conjugate vaccines in Finland. Rev Med Microbiol 1996;7:23141. [3] Hargreaves R, Slack M, Howard A, Anderson E, Ramsay M. Changing patterns of invasive Haemophilus inuenzae disease in England and Wales after introduction of the Hib vaccination programme. BMJ 1996;312:1601.
292
P.H. Mkel et al. / Vaccine 22 (2003) 287292 [16] Kyhty H, Eskola J, Peltola H, et al. Immunogenicity in infants of a vaccine composed of Haemophilus inuenzae type b capsular polysaccharide mixed with DPT or conjugated to diphtheria toxoid. J Infect Dis 1987;155:1006. [17] Eskola J, Peltola H, Mkel P, et al. Antibody levels achieved in infants by course of Haemophilus inuenzae type b polysaccharide/ diphtheria toxoid conjugate vaccine. Lancet 1985;i:11846. [18] Mkel P, Peltola H, Kyhty H, et al. Polysaccharide vaccines of group A Neisseria meningitidis and Haemophilus inuenzae type b. J Infect Dis 1977;136:S4350. [19] Kyhty H, Eskola J, Peltola H, Rnnberg PR, Kela E, Karanko V. Antibody response to four Haemophilus inuenzae type b conjugate vaccines. Am J Dis Children 1991;145:2237. [20] Phipps D, West J, Eby R, Koster M, Madore D, Quataert S. An ELISA employing a Haemophilus inuenzae type b oligosaccharidehuman serum albumin conjugate correlates with radioantigen binding assay. J Immunol Methods 1990;135:1218. [21] Goldblatt D, Pinto Vaz A, Miller E. Antibody avidity as a surrogate marker of successful priming by Haemophilus inuenzae type b conjugate vaccines following infant immunisation. J Infect Dis 1998;177:11125. [22] Anttila M, Eskola J, hman H, Kyhty H. Avidity of IgG for Streptococcus Pneumoniae type 6B and 23F polysaccharides in infants primed with pneumococcal conjugates and boosted with polysaccharide or conjugate vaccines. J Infect Dis 1998;177: 161421. [23] Claesson B, Trollfors B, Anderson P, et al. Serum antibodies in 6-year-old children vaccinated in infancy with a Haemophilus inuenzae type btetanus toxoid conjugate vaccine. Pediatr Infect Dis J 1996;15:1702. [24] Heath P, Bowen-Morris J, Grifths D, Grifths H, Crook D, Moxon E. Antibody persistence and Haemophilus inuenzae type b carriage after infant immunisation with PRP-T. Arch Dis Childhood 1997;77:48892. [25] Scheifele D, Halperin S, Guasparini R, Meekison W, Pim CLB. Extended follow-up of antibody levels and antigen responsiveness after two Haemophilus inuenzae type b conjugate vaccines. J Pediatr 1991;35:2405. [26] van den Hof S, de Melker E, Berbers G, van der Kraak P, Conyn-van Spaendonck M. Antibodies to Haemophilus inuenzae serotype b in The Netherlands a few years after the introduction of routine vaccination. CID 2001;32:28. [27] Auranen K. Backcalculating the age-specic incidence of recurrent subclinical Haemophilus inuenzae type b infection. Stat Med 2000;19:28196.
[4] Adams W, Deaver K, Colchi S, Plikaytis B, Zell E, Broome C, et al. Decline in childhood Haemophilus inuenzae type b (Hib) disease in the Hib vaccine era. JAMA 1993;269:2216. [5] Bradshaw M, Schneerson R, Parke J, Robbins J. Bacterial antigens cross-reactive with the capsular polysaccharide of Haemophilus inuenzae type b. Lancet 1971;i:10957. [6] Schneerson R, Bradshaw M, Whisnant J, Myerowitz R, Parke J, Robbins J. An Escherichia coli antigen cross-reactive with the capsular polysacharide of Haemophilus inuenzae type b: occurrence among known serotypes, and immunochemical and biological properties of E. coli antisera toward H. inuenzae type b. J Immunol 1972;108:155162. [7] Robbins J, Schneerson R, Glode M, et al. Cross-reactive antigens and immunity to disease caused by encapsulated bacteria. J Allergy Clin Immunol 1975;56:14151. [8] Peltola H, Kyhty H, Sivonen A, Mkel P. Haemophilus inuenzae type b capsular polysaccharide vaccine in children: a double-blind eld study of 100 000 vaccinees 3 months to 5 years of age in Finland. Pediatrics 1977;60:7307. [9] Kyhty H, Peltola H, Karanko V, Mkel P. The protective level of serum antibodies to the capsular polysaccharide of Haemophilus inuenzae type b. J Infect Dis 1983;147:1100. [10] Robbins J, Parke JJ, Schneerson R, Wishnant J. Quantitative measurement of natural and immunisation-induced Haemophilus inuenzae type b capsular polysaccharide antibodies. Pediat Res 1973;7:10310. [11] Auranen K, Eichner M, Kyhty H, Takala A, Arjas E. A hierarchical Bayesian model to predict the duration of immunity to Hib. Biometrics 1999;55:130613. [12] Leino T, Auranen K, Mkel P, Kyhty H, Takala A. Dynamics of natural immunity caused by subclinical infections, case study on Haemophilus inuenzae type b (Hib). Epidemiol Infect 2000;125:58391. [13] Kyhty H, Eskola J, Peltola H, Saarinen L, Mkel P. High antibody responses to booster doses of either Haemophilus inuenzae type b capsular polysaccharide or conjugate vaccine after primary immunizations with conjugate vaccine. I. Infect Dis 1992;16: S1656. [14] Granoff D, Holmes S, Osterholm M, et al. Induction of immunologic memory in infants primed with Haemophilus inuenzae type b conjugate vaccines. J Infect Dis 1993;168:66371. [15] Einhorn M, Wienberg G, Anderson E, Granoff P, Granoff D. Immunogenicity in infants of Haemophilus inuenzae type b polysaccharide in a conjugate vaccine with Neisseria meningitidis outer-membrane protein. Lancet 1986;9:299302.
Você também pode gostar
- Police CodesDocumento8 páginasPolice Codesrlh2022100% (3)
- AGREEMENT ON AN INTERNATIONAL ENERGY PROGRAM (As Amended 9 May 2014)Documento116 páginasAGREEMENT ON AN INTERNATIONAL ENERGY PROGRAM (As Amended 9 May 2014)rlh2022Ainda não há avaliações
- Police CodesDocumento8 páginasPolice Codesrlh2022100% (3)
- Biologicaql and Medical MeasurementsDocumento8 páginasBiologicaql and Medical Measurementsrlh2022Ainda não há avaliações
- Pseudo History and PseudocienceDocumento18 páginasPseudo History and Pseudociencerlh2022Ainda não há avaliações
- Healthy and Sustainable Habitat in ColombiaDocumento23 páginasHealthy and Sustainable Habitat in ColombiaFernando Michaels100% (1)
- The Science Behind LumosityDocumento21 páginasThe Science Behind Lumositydevang_33Ainda não há avaliações
- Linear Algebra 66808660Documento84 páginasLinear Algebra 66808660rlh2022Ainda não há avaliações
- Parapsichology RussianDocumento15 páginasParapsichology Russianrlh2022Ainda não há avaliações
- Healthy and Sustainable Habitat in ColombiaDocumento23 páginasHealthy and Sustainable Habitat in ColombiaFernando Michaels100% (1)
- Alternative MedicineDocumento13 páginasAlternative Medicinerlh2022Ainda não há avaliações
- PlantsDocumento693 páginasPlantsrlh2022100% (2)
- Niveles de AnticuerposDocumento10 páginasNiveles de Anticuerposrlh2022Ainda não há avaliações
- Obama Hypnosis: A Theory by The RightDocumento67 páginasObama Hypnosis: A Theory by The Rightpappalardo100% (2)
- Human Uniqueness and Theoretical ContentDocumento20 páginasHuman Uniqueness and Theoretical Contentrlh2022Ainda não há avaliações
- Chemistry For Environmental Professionals Outline of Lectures (Tentative)Documento1 páginaChemistry For Environmental Professionals Outline of Lectures (Tentative)rlh2022Ainda não há avaliações
- ReferencesDocumento2 páginasReferencesrlh2022Ainda não há avaliações
- IntroDocumento43 páginasIntrorlh2022Ainda não há avaliações
- Evidence For Connsciuousnessrelateda Anomalies in Random Physical SyustemsDocumento16 páginasEvidence For Connsciuousnessrelateda Anomalies in Random Physical Syustemsrlh2022Ainda não há avaliações
- ResourcesDocumento3 páginasResourcesrlh2022Ainda não há avaliações
- Environmental ChemistryDocumento3 páginasEnvironmental Chemistryrlh2022Ainda não há avaliações
- Course Booklet July 2011Documento42 páginasCourse Booklet July 2011rlh2022Ainda não há avaliações
- Chemistry in The EnvironmentDocumento3 páginasChemistry in The Environmentrlh2022Ainda não há avaliações
- The Toxicity of RDX To The Freshwater Green Alga Selenastrum CapricornutumDocumento9 páginasThe Toxicity of RDX To The Freshwater Green Alga Selenastrum Capricornutumrlh2022Ainda não há avaliações
- Toxicity MercurioDocumento8 páginasToxicity Mercuriorlh2022Ainda não há avaliações
- Removing Heavy Metals From Waste WaterDocumento21 páginasRemoving Heavy Metals From Waste Waterrlh2022100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- How Jan Koum became a billionaire internet entrepreneurDocumento20 páginasHow Jan Koum became a billionaire internet entrepreneurfin99Ainda não há avaliações
- Jessica Evans Epi PaperDocumento12 páginasJessica Evans Epi Paperapi-439893609Ainda não há avaliações
- Annex 4 Cat RonaldDocumento7 páginasAnnex 4 Cat Ronaldrkvance5100% (1)
- Interview With Barbara Loe Fisher On IOM Report 2011Documento11 páginasInterview With Barbara Loe Fisher On IOM Report 2011Fadhli QuzwainAinda não há avaliações
- (PDF) MMDSTDocumento50 páginas(PDF) MMDSTJan Oliver YaresAinda não há avaliações
- Learning From AEFI SurveillanceDocumento46 páginasLearning From AEFI SurveillanceAgus JunaidiAinda não há avaliações
- 2019 AUG 7 Phe Epidemiological Update MeaslesDocumento10 páginas2019 AUG 7 Phe Epidemiological Update MeaslesJENIFFER NATALY ALVAREZ GALINDOAinda não há avaliações
- Integrated Management of Childhood Illness: Child Aged 2 Months Up To 5 YearsDocumento44 páginasIntegrated Management of Childhood Illness: Child Aged 2 Months Up To 5 YearsJulio Iñigo López100% (22)
- Catchup Schedule PR PDFDocumento2 páginasCatchup Schedule PR PDFGama Adi SafutraAinda não há avaliações
- Welcome Back 2014 - Mooresville TribuneDocumento48 páginasWelcome Back 2014 - Mooresville TribuneMatthew HensleyAinda não há avaliações
- BordetellaDocumento54 páginasBordetellatummalapalli venkateswara rao100% (2)
- Dengue Prevention Awareness Among The Residents of Woodhouse St. Gordon HeightsDocumento35 páginasDengue Prevention Awareness Among The Residents of Woodhouse St. Gordon HeightsRod Daniel CalistonAinda não há avaliações
- Clearance ChecklistDocumento2 páginasClearance ChecklistJasminKerreUllamotVillarinAinda não há avaliações
- Following VaccinationsDocumento117 páginasFollowing VaccinationsDumitruAinda não há avaliações
- Importance of ImmunizationDocumento3 páginasImportance of ImmunizationEsteban JuanAinda não há avaliações
- Mandatory VaccinationsDocumento7 páginasMandatory Vaccinationsapi-487208181Ainda não há avaliações
- BPL HistoryDocumento14 páginasBPL HistoryTim SandleAinda não há avaliações
- The Andrew Wakefield CaseDocumento3 páginasThe Andrew Wakefield Caseapi-202268486Ainda não há avaliações
- Vaccinations Argumentative Essay - Lyla AlmoninaDocumento3 páginasVaccinations Argumentative Essay - Lyla Almoninaapi-4441503820% (1)
- Vaccine Storage LabelsDocumento17 páginasVaccine Storage LabelsNessax33Ainda não há avaliações
- Varicella Zooster VirusDocumento9 páginasVaricella Zooster VirusChikita Artia SariAinda não há avaliações
- Lifeline Health Insurance Plan SummaryDocumento84 páginasLifeline Health Insurance Plan SummaryJayesh KillekarAinda não há avaliações
- Table I IAP Immunization Schedule 2016 FinalDocumento7 páginasTable I IAP Immunization Schedule 2016 FinalVaishnavi AgrawalAinda não há avaliações
- P-Form Weekly Idsp Alert - Week 05 BANASKANTHA PALANPURDocumento10 páginasP-Form Weekly Idsp Alert - Week 05 BANASKANTHA PALANPURPankaj ModhAinda não há avaliações
- Extent of Compliance To Immunization Reasons For Non Continuity and Its Consequences PDFDocumento26 páginasExtent of Compliance To Immunization Reasons For Non Continuity and Its Consequences PDFAPRIL LYNAinda não há avaliações
- "Expanded Program On Immunization": Angeles University FoundationDocumento12 páginas"Expanded Program On Immunization": Angeles University FoundationJaillah Reigne CuraAinda não há avaliações
- WEDALDocumento1 páginaWEDALJitu YadavAinda não há avaliações
- Case Night BlindnessDocumento3 páginasCase Night BlindnessNovie Bagayan100% (1)
- Environmental monitoring of clean rooms in vaccine manufacturing facilitiesDocumento37 páginasEnvironmental monitoring of clean rooms in vaccine manufacturing facilitiesKrischaireddy AnnapureddyAinda não há avaliações
- Paez - Unit 9Documento2 páginasPaez - Unit 9tatianaAinda não há avaliações