Você também pode gostar
- Parenteral Products: The Preparation and Quality Control of Products for InjectionNo EverandParenteral Products: The Preparation and Quality Control of Products for InjectionAinda não há avaliações
- Formulation and Evaluation of Floating Tablet of Captopril: Sameer Singh, Kalpana Prajapati, A K Pathak, A MishraDocumento9 páginasFormulation and Evaluation of Floating Tablet of Captopril: Sameer Singh, Kalpana Prajapati, A K Pathak, A Mishraamalia shaldaAinda não há avaliações
- My Research PaperDocumento10 páginasMy Research PaperMamta AroraAinda não há avaliações
- A C A D e M I C S C I e N C e SDocumento6 páginasA C A D e M I C S C I e N C e SKris Natalia ManihurukAinda não há avaliações
- JPSR 03110106Documento9 páginasJPSR 03110106sunilpdAinda não há avaliações
- Formulation and Evaluation of Transdermal Patch of Repaglinide PDFDocumento9 páginasFormulation and Evaluation of Transdermal Patch of Repaglinide PDFapa menAinda não há avaliações
- IJPSR LibreDocumento5 páginasIJPSR LibreWahyu RedfieldAinda não há avaliações
- International Journal of Pharma and Bio Sciences V1 (2) 2010Documento10 páginasInternational Journal of Pharma and Bio Sciences V1 (2) 2010Desy Ratna Sari NainggolanAinda não há avaliações
- HPMCP & Cap As Enteric Coated &chitosan As Sustained ReleaseDocumento9 páginasHPMCP & Cap As Enteric Coated &chitosan As Sustained ReleasejackbahlulAinda não há avaliações
- Formulation Development and Evaluation of Pantoprazole Delayed Release TabletsDocumento13 páginasFormulation Development and Evaluation of Pantoprazole Delayed Release TabletsAnish Kumar A0% (1)
- Jurnal SIODocumento8 páginasJurnal SIOTaufik HaldiAinda não há avaliações
- International Journal of Research in Pharmacy and ScienceDocumento10 páginasInternational Journal of Research in Pharmacy and ScienceAat Prayoga MuhtarAinda não há avaliações
- Formulation and Evaluation of Montelukast Sodium and Levocetirizine Dihydrochloride Sublingual TabletsDocumento5 páginasFormulation and Evaluation of Montelukast Sodium and Levocetirizine Dihydrochloride Sublingual TabletsNeerajAinda não há avaliações
- Folic 5 MG FormDocumento6 páginasFolic 5 MG FormChandan SinghAinda não há avaliações
- Formulation and Evaluation of Quinapril Sustained Release Matrix TabletsDocumento14 páginasFormulation and Evaluation of Quinapril Sustained Release Matrix TabletsSyed Qasim MehmoodAinda não há avaliações
- Formulation, Evaluation, and Comparison of Bilayered and Multilayered Mucoadhesive Buccal Devices of Propranolol HydrochlorideDocumento8 páginasFormulation, Evaluation, and Comparison of Bilayered and Multilayered Mucoadhesive Buccal Devices of Propranolol HydrochlorideNarendra BhupatiAinda não há avaliações
- Development and Optimization of Fast Dissolving Tablet of Levocetrizine HCLDocumento10 páginasDevelopment and Optimization of Fast Dissolving Tablet of Levocetrizine HCLmariohuangAinda não há avaliações
- Pre Thesis PresentationDocumento23 páginasPre Thesis Presentationsyed azeemAinda não há avaliações
- Experiment No:: Object/AimDocumento9 páginasExperiment No:: Object/AimSudeep KothariAinda não há avaliações
- Formulation and Evaluation of Orally Disintegrating Tablets of SertralineDocumento7 páginasFormulation and Evaluation of Orally Disintegrating Tablets of SertralineDinesh BabuAinda não há avaliações
- Core and CupDocumento9 páginasCore and CupVikas JhawatAinda não há avaliações
- Development and Characterization of Orally Disintegrating Tablets Containing A Captopril-Cyclodextrin ComplexDocumento19 páginasDevelopment and Characterization of Orally Disintegrating Tablets Containing A Captopril-Cyclodextrin ComplexValentina AnutaAinda não há avaliações
- Formulation and Evaluation of Floating Tablet of Metoprolol SuccinateDocumento13 páginasFormulation and Evaluation of Floating Tablet of Metoprolol SuccinateEditor IJTSRDAinda não há avaliações
- DiltiazemDocumento10 páginasDiltiazemSari Puspita DewiAinda não há avaliações
- Pharmaceutical Characterization and Assessment of Drug Release Behaviour of Diclofenac Sodium Extended Release Matrix DevicesDocumento8 páginasPharmaceutical Characterization and Assessment of Drug Release Behaviour of Diclofenac Sodium Extended Release Matrix DevicesnikhilsachanAinda não há avaliações
- MucoadhesifDocumento26 páginasMucoadhesifFeny RafnasariAinda não há avaliações
- DuocapDocumento4 páginasDuocaplouish9175841Ainda não há avaliações
- JPRHC: Research ArticleDocumento9 páginasJPRHC: Research Articleabhijit_gothoskar6039Ainda não há avaliações
- International Journal of PharmacyDocumento6 páginasInternational Journal of Pharmacygthic.underAinda não há avaliações
- Higuchi ModelDocumento6 páginasHiguchi ModelSantanu MallikAinda não há avaliações
- Design, Evaluation and Study of Effect of Hydrophilic Polymers On Release Rate of Antiulcer Floating TabletsDocumento10 páginasDesign, Evaluation and Study of Effect of Hydrophilic Polymers On Release Rate of Antiulcer Floating TabletsnenavathkumarAinda não há avaliações
- 24315-Article Text-87444-1-10-20150726Documento6 páginas24315-Article Text-87444-1-10-20150726AnditapitalokaAinda não há avaliações
- Stamford Journal of Pharmaceutical SciencesDocumento6 páginasStamford Journal of Pharmaceutical SciencesEr RicitosAinda não há avaliações
- 1246 PDFDocumento4 páginas1246 PDFPrima RiyandiAinda não há avaliações
- Abu Afzal Mohammad Shakar Et Al (2012)Documento6 páginasAbu Afzal Mohammad Shakar Et Al (2012)neil_vidhyaAinda não há avaliações
- Formulation Development and Evaluation of Famotidine Floating TabletDocumento6 páginasFormulation Development and Evaluation of Famotidine Floating TabletCang HaedarAinda não há avaliações
- Bilayered Transmucosal Drug Delivery System of Pravastatin Sodium: Statistical Optimization, in and Stability AssessmentDocumento14 páginasBilayered Transmucosal Drug Delivery System of Pravastatin Sodium: Statistical Optimization, in and Stability AssessmentfadillaAinda não há avaliações
- Literature ReviewDocumento10 páginasLiterature Review006giriAinda não há avaliações
- Evaluation of TabletsDocumento8 páginasEvaluation of TabletsPraneeth Reddy100% (8)
- Jurnal Transdermal IbuprofenDocumento12 páginasJurnal Transdermal IbuprofenRatissa Eka NingtiyasAinda não há avaliações
- Jurnal CarbamazepinDocumento9 páginasJurnal CarbamazepinRosamaria Yuni UtamiAinda não há avaliações
- A C A D e M I C S C I e N C e SDocumento5 páginasA C A D e M I C S C I e N C e SlovehopeAinda não há avaliações
- Pulsatile Dds PDFDocumento19 páginasPulsatile Dds PDFSiva PrasadAinda não há avaliações
- Article WJPR 1399543685Documento14 páginasArticle WJPR 1399543685Nafi Hasan ZahidAinda não há avaliações
- AcyclovirtabletsDocumento4 páginasAcyclovirtabletsdonsoucy1069Ainda não há avaliações
- Formulation and Evaluation of Metformin Hydrochloride Floating Tablets Using Gum KondagoguDocumento1 páginaFormulation and Evaluation of Metformin Hydrochloride Floating Tablets Using Gum Kondagogumarslk1Ainda não há avaliações
- Ajptr8gholves BDocumento11 páginasAjptr8gholves BChương PhanAinda não há avaliações
- Admin, Journal Manager, 823Documento7 páginasAdmin, Journal Manager, 823vijay mAinda não há avaliações
- Design, Development of Formulation of Eperisone Hydrochrodide Floating Sustain Realease Tablet and Its EvaluationDocumento22 páginasDesign, Development of Formulation of Eperisone Hydrochrodide Floating Sustain Realease Tablet and Its EvaluationabhitavAinda não há avaliações
- Effect of Superdisintegrating Agent and Osmogens On Ciprofloxacin Loaded Naturally Occurring Biodegradable Coated Tablets For Colon TargetingDocumento6 páginasEffect of Superdisintegrating Agent and Osmogens On Ciprofloxacin Loaded Naturally Occurring Biodegradable Coated Tablets For Colon TargetingsuparshyaAinda não há avaliações
- Orange PeelDocumento5 páginasOrange Peellalit4u78Ainda não há avaliações
- Ijpir 16 403 - 98 110Documento13 páginasIjpir 16 403 - 98 110JeffAinda não há avaliações
- 223 PDFDocumento9 páginas223 PDF26nazilarenoatAinda não há avaliações
- 4.kalpana ArticleDocumento5 páginas4.kalpana ArticleBaru Chandrasekhar RaoAinda não há avaliações
- Franz Diffusion Cell Approach For Pre-Formulation Characterisation of Ketoprofen Semi-Solid Dosage FormsDocumento8 páginasFranz Diffusion Cell Approach For Pre-Formulation Characterisation of Ketoprofen Semi-Solid Dosage FormsHEMAAinda não há avaliações
- Paper 2Documento8 páginasPaper 2jodiAinda não há avaliações
- Candesartan Cilecetil Formula Dry GranulationDocumento8 páginasCandesartan Cilecetil Formula Dry GranulationnandaAinda não há avaliações
- Formulation and Evaluation of Verapamil Hydrochloride Buccoadhesive TabletsDocumento10 páginasFormulation and Evaluation of Verapamil Hydrochloride Buccoadhesive TabletsRiri MonicaAinda não há avaliações
- Formulation and Evaluation of Controlled Release Ocular Inserts of Betaxolol HydrochlorideDocumento5 páginasFormulation and Evaluation of Controlled Release Ocular Inserts of Betaxolol HydrochlorideIOSR Journal of PharmacyAinda não há avaliações
- 125557353Documento5 páginas125557353Mira TjakkuduAinda não há avaliações
- Sulfur Vulcanization of Natural Rubber - Reaction Mechanisms and Kinetic PDFDocumento102 páginasSulfur Vulcanization of Natural Rubber - Reaction Mechanisms and Kinetic PDFchristopher_kephart1Ainda não há avaliações
- Guidance For The Implementation of A Quality Management System in Drug Testing LaboratoriesDocumento50 páginasGuidance For The Implementation of A Quality Management System in Drug Testing LaboratoriesamirnimoAinda não há avaliações
- Criterios DM Seguan Ada 2011Documento8 páginasCriterios DM Seguan Ada 2011Ricardo JuarezAinda não há avaliações
- Effect of Aceclofenac On Pharmacokinetic of PhenytoinDocumento5 páginasEffect of Aceclofenac On Pharmacokinetic of PhenytoinMira TjakkuduAinda não há avaliações
- Effect of Aceclofenac On Pharmacokinetic of PhenytoinDocumento5 páginasEffect of Aceclofenac On Pharmacokinetic of PhenytoinMira TjakkuduAinda não há avaliações
- Probit 2Documento5 páginasProbit 2Mira TjakkuduAinda não há avaliações
- ASEAN Stability GuidelineDocumento37 páginasASEAN Stability GuidelinevarizzzAinda não há avaliações
- In Vitro in Vivo: CorrelationsDocumento21 páginasIn Vitro in Vivo: CorrelationsBandameedi RamuAinda não há avaliações
- Dogs-Ketamine-Diazepam-Induction DosageDocumento2 páginasDogs-Ketamine-Diazepam-Induction DosageArun NAinda não há avaliações
- Walter Modell M. D., F.A.C.P., Doris J. Place R. N. (Auth.) - The Use of Drugs - Principles of Pharmacology and Therapeutics For Nurses (1957, Springer-Verlag Berlin Heidelberg) PDFDocumento350 páginasWalter Modell M. D., F.A.C.P., Doris J. Place R. N. (Auth.) - The Use of Drugs - Principles of Pharmacology and Therapeutics For Nurses (1957, Springer-Verlag Berlin Heidelberg) PDFbluegreenalgaAinda não há avaliações
- Obat IFARSDocumento5 páginasObat IFARSOky Spinola IdroosAinda não há avaliações
- DurDocumento18 páginasDurxtremist2001100% (2)
- Opioid Conversion Chart 2020 1Documento1 páginaOpioid Conversion Chart 2020 1aengus42Ainda não há avaliações
- National Drug Take Back Day ScheduleDocumento2 páginasNational Drug Take Back Day ScheduleWVLT NewsAinda não há avaliações
- Daftar Obat-Obatan Rumah Sakit AzzahraDocumento12 páginasDaftar Obat-Obatan Rumah Sakit Azzahraelimawati elimawatiAinda não há avaliações
- List Obat Pengobatan MassalDocumento4 páginasList Obat Pengobatan MassaldryusiaspanAinda não há avaliações
- True/False: CHAPTER 3 Pharmokinetics: The Absorption, Distribution, and Excretion of DrugsDocumento2 páginasTrue/False: CHAPTER 3 Pharmokinetics: The Absorption, Distribution, and Excretion of Drugsbelinchon96Ainda não há avaliações
- 4V8T3XZT ManufacturingUnitDocumento7 páginas4V8T3XZT ManufacturingUnitGuru KrupaAinda não há avaliações
- 50 Q&A Zinc Sulfate Tablets - Nov2016 PDFDocumento5 páginas50 Q&A Zinc Sulfate Tablets - Nov2016 PDFSunil Murkikar (GM - PMI Quality Operations)Ainda não há avaliações
- Core and CupDocumento9 páginasCore and CupVikas JhawatAinda não há avaliações
- Drug Development: FDA's Definition of A New DrugDocumento11 páginasDrug Development: FDA's Definition of A New DrugSophie MendezAinda não há avaliações
- PrescriptionsDocumento6 páginasPrescriptionsChiela Alcantara BagnesAinda não há avaliações
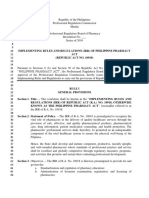
- IRR Implementing Rules and Regulations of Philippine Irr of Ra10918 090916epdfDocumento42 páginasIRR Implementing Rules and Regulations of Philippine Irr of Ra10918 090916epdfDenise Marfe PedregosaAinda não há avaliações
- Abstract - Docx ALLDocumento138 páginasAbstract - Docx ALLvivekAinda não há avaliações
- 1b SPC PL Metomotyl 10 MG Chew Tab Final CleanDocumento16 páginas1b SPC PL Metomotyl 10 MG Chew Tab Final CleanPhuong Anh BuiAinda não há avaliações
- MCQ 2 - PharmacodynamicsDocumento5 páginasMCQ 2 - PharmacodynamicsHillary Nguyen100% (3)
- Registered Medicine List 07-04-2014 Sse Frequently UpdatedDocumento116 páginasRegistered Medicine List 07-04-2014 Sse Frequently Updatedjema; belihuAinda não há avaliações
- Daftar Obat Emergency KitDocumento8 páginasDaftar Obat Emergency KitvidyaAinda não há avaliações
- Pharma Assignment 2Documento7 páginasPharma Assignment 2Angelica VillalonAinda não há avaliações
- Ampoules and Vials: Drugs DrugsDocumento1 páginaAmpoules and Vials: Drugs DrugsHeba HanyAinda não há avaliações
- Pharmacology: An Introduction: Pharmacology Dr. Abdul Salam NazmiDocumento18 páginasPharmacology: An Introduction: Pharmacology Dr. Abdul Salam NazmirimazkhanAinda não há avaliações
- Dexametasone: No Nama Obat Sediaan Jumlah Satua N Harga Beli Harga JualDocumento1 páginaDexametasone: No Nama Obat Sediaan Jumlah Satua N Harga Beli Harga Jualfebri12Ainda não há avaliações
- Lplpo Agustus 2017Documento66 páginasLplpo Agustus 2017Selly Wijaya BermawiAinda não há avaliações
- Glenmark Becomes The First Pharmaceut Cal Company in India To ReceiveDocumento2 páginasGlenmark Becomes The First Pharmaceut Cal Company in India To ReceiveManmohan TiwariAinda não há avaliações
- KPJ Healthcare University CollegeDocumento95 páginasKPJ Healthcare University CollegeArchanah Rajamanikam50% (2)
- Molecular Docking in Structure-Based Drug DesignDocumento33 páginasMolecular Docking in Structure-Based Drug DesignIvan Tubert-BrohmanAinda não há avaliações
- The Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookNo EverandThe Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookAinda não há avaliações
- Physical and Chemical Equilibrium for Chemical EngineersNo EverandPhysical and Chemical Equilibrium for Chemical EngineersNota: 5 de 5 estrelas5/5 (1)
- Process Plant Equipment: Operation, Control, and ReliabilityNo EverandProcess Plant Equipment: Operation, Control, and ReliabilityNota: 5 de 5 estrelas5/5 (1)
- Guidelines for the Management of Change for Process SafetyNo EverandGuidelines for the Management of Change for Process SafetyAinda não há avaliações
- Nuclear Energy in the 21st Century: World Nuclear University PressNo EverandNuclear Energy in the 21st Century: World Nuclear University PressNota: 4.5 de 5 estrelas4.5/5 (3)
- Process Steam Systems: A Practical Guide for Operators, Maintainers, and DesignersNo EverandProcess Steam Systems: A Practical Guide for Operators, Maintainers, and DesignersAinda não há avaliações
- The Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookNo EverandThe Periodic Table of Elements - Alkali Metals, Alkaline Earth Metals and Transition Metals | Children's Chemistry BookAinda não há avaliações
- Well Control for Completions and InterventionsNo EverandWell Control for Completions and InterventionsNota: 4 de 5 estrelas4/5 (10)
- An Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksNo EverandAn Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksNota: 5 de 5 estrelas5/5 (1)
- Guidelines for Chemical Process Quantitative Risk AnalysisNo EverandGuidelines for Chemical Process Quantitative Risk AnalysisNota: 5 de 5 estrelas5/5 (1)
- Pharmaceutical Blending and MixingNo EverandPharmaceutical Blending and MixingP. J. CullenNota: 5 de 5 estrelas5/5 (1)
- Principles and Case Studies of Simultaneous DesignNo EverandPrinciples and Case Studies of Simultaneous DesignAinda não há avaliações
- Piping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationNo EverandPiping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationNota: 4 de 5 estrelas4/5 (18)
- Operational Excellence: Journey to Creating Sustainable ValueNo EverandOperational Excellence: Journey to Creating Sustainable ValueAinda não há avaliações
- Guidelines for Engineering Design for Process SafetyNo EverandGuidelines for Engineering Design for Process SafetyAinda não há avaliações
- Sodium Bicarbonate: Nature's Unique First Aid RemedyNo EverandSodium Bicarbonate: Nature's Unique First Aid RemedyNota: 5 de 5 estrelas5/5 (21)
- Understanding Process Equipment for Operators and EngineersNo EverandUnderstanding Process Equipment for Operators and EngineersNota: 4.5 de 5 estrelas4.5/5 (3)
- The HAZOP Leader's Handbook: How to Plan and Conduct Successful HAZOP StudiesNo EverandThe HAZOP Leader's Handbook: How to Plan and Conduct Successful HAZOP StudiesAinda não há avaliações
- Chemical Process Safety: Learning from Case HistoriesNo EverandChemical Process Safety: Learning from Case HistoriesNota: 4 de 5 estrelas4/5 (14)
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsNo EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsAinda não há avaliações