Você também pode gostar
- Infective Endocarditis: A Multidisciplinary ApproachNo EverandInfective Endocarditis: A Multidisciplinary ApproachArman KilicAinda não há avaliações
- Dexmedetomidine Expanding Role in AnesthesiaDocumento9 páginasDexmedetomidine Expanding Role in AnesthesiaUnggul Yudha100% (1)
- Dexmedetomidine: (Precedex - Abbott Laboratories)Documento6 páginasDexmedetomidine: (Precedex - Abbott Laboratories)battreyAinda não há avaliações
- Clinical Use of DexmedetomidineDocumento29 páginasClinical Use of DexmedetomidineAnil SathyadasAinda não há avaliações
- A Comparative Study of Clonidine and Lignocaine For Attenuating Pressor Responses To Laryngoscopy and Endotracheal Intubation in Neurosurgical CasesDocumento5 páginasA Comparative Study of Clonidine and Lignocaine For Attenuating Pressor Responses To Laryngoscopy and Endotracheal Intubation in Neurosurgical Casesnethra nitinAinda não há avaliações
- General Anesthetics AbeerDocumento45 páginasGeneral Anesthetics AbeerYousef JafarAinda não há avaliações
- Cikini Pengelolaan Nyeri FinalDocumento85 páginasCikini Pengelolaan Nyeri FinalisabellaruthhhAinda não há avaliações
- Muscle RelaxantDocumento42 páginasMuscle RelaxantMirza Shaharyar BaigAinda não há avaliações
- Tumor Med TysDocumento21 páginasTumor Med TysTias DiahAinda não há avaliações
- Essential Tremor Diagnosis and TreatmentDocumento32 páginasEssential Tremor Diagnosis and TreatmentAntony JebarajAinda não há avaliações
- ACute Pain Management Transforming Evidence Into PracticeDocumento60 páginasACute Pain Management Transforming Evidence Into PracticeSurjya UpadhyayAinda não há avaliações
- Evaluation and Management of Elevated Intracranial Pressure in AdultsDocumento28 páginasEvaluation and Management of Elevated Intracranial Pressure in AdultssandykumalaAinda não há avaliações
- Neuroleptic Malignant SyndromeDocumento19 páginasNeuroleptic Malignant SyndromeFauzi TsanifiandiAinda não há avaliações
- Postoperative Pain ManagementDocumento43 páginasPostoperative Pain ManagementPingKikiAinda não há avaliações
- Anesthesia CHD Non Cardiac SurgeryDocumento97 páginasAnesthesia CHD Non Cardiac SurgeryDon DavidAinda não há avaliações
- Neuroleptic Malignant SyndromeDocumento18 páginasNeuroleptic Malignant Syndromedrkadiyala2Ainda não há avaliações
- ACUTE CONFUSIONAL STATE KoreksiDocumento39 páginasACUTE CONFUSIONAL STATE KoreksiMuhammad Afief100% (1)
- 2 PneumoniaDocumento53 páginas2 PneumoniaLucyellowOttemoesoeAinda não há avaliações
- Post Op AnalgesiaDocumento2 páginasPost Op AnalgesiaTom MallinsonAinda não há avaliações
- Perioperative Pain Management in Trauma PatientsDocumento22 páginasPerioperative Pain Management in Trauma Patientsblack pink in ur area 21Ainda não há avaliações
- Drug Therapy For Parkinson's DiseaseDocumento9 páginasDrug Therapy For Parkinson's DiseaseDireccion Medica EJEAinda não há avaliações
- Inhalational AnesthesiaDocumento96 páginasInhalational AnesthesiaNachee PatricioAinda não há avaliações
- General AnestheticsDocumento36 páginasGeneral AnestheticsnidyaAinda não há avaliações
- The Hepatorenal SyndromeDocumento26 páginasThe Hepatorenal SyndromeWaraBawanaAinda não há avaliações
- Lecture: Adrenal DisordersDocumento78 páginasLecture: Adrenal DisordersOchendo KingxAinda não há avaliações
- Anaesthesia in Liver Disease PatientDocumento49 páginasAnaesthesia in Liver Disease PatientVG FernandezAinda não há avaliações
- Acute Confusional State ManagementDocumento18 páginasAcute Confusional State ManagementAhmed AbdelgelilAinda não há avaliações
- Midazolam FinalDocumento2 páginasMidazolam FinalAhmad AbqariAinda não há avaliações
- Hyporeninemic HypoaldosteronismDocumento12 páginasHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisAinda não há avaliações
- Pseudomonad GroupDocumento18 páginasPseudomonad GroupNikita MarieAinda não há avaliações
- WHO Analgesic LadderDocumento2 páginasWHO Analgesic LadderAndi PakdheeAinda não há avaliações
- CKDDocumento54 páginasCKDAnonymous UHnQSkxLBDAinda não há avaliações
- Adult Chemotherapy Induced Anaphylaxis PolicyDocumento12 páginasAdult Chemotherapy Induced Anaphylaxis PolicyMohammed Gazo100% (1)
- TLS FinalDocumento69 páginasTLS FinalGrace Arthur100% (1)
- Assignment AnesthesiaDocumento9 páginasAssignment AnesthesiaRavi PatelAinda não há avaliações
- Epidural Anesthesia (OB)Documento3 páginasEpidural Anesthesia (OB)zooAinda não há avaliações
- Eff Pleura & PneumothoraxDocumento69 páginasEff Pleura & PneumothoraxUswatun Hasanah RIAinda não há avaliações
- Radio PharmaceuticalsDocumento48 páginasRadio PharmaceuticalsKris Joy EbonAinda não há avaliações
- Adrenergic DrugsDocumento33 páginasAdrenergic DrugsZsa Zsa FebryanaAinda não há avaliações
- Dopamine Antagonists in ICU DeliriumDocumento2 páginasDopamine Antagonists in ICU DeliriumRodrigoSachiFreitasAinda não há avaliações
- Neuroleptic Malignant Syndrome MedscapeDocumento9 páginasNeuroleptic Malignant Syndrome MedscapeEra SulistiyaAinda não há avaliações
- Delirium in Critically IllDocumento37 páginasDelirium in Critically IllSanj.etcAinda não há avaliações
- Adverse Drug Reactions (ADRS)Documento24 páginasAdverse Drug Reactions (ADRS)ANAM IQBALAinda não há avaliações
- Psychosis ThesisDocumento19 páginasPsychosis ThesisjustoneoftheguysAinda não há avaliações
- Epidural Hematoma: Kurniasari Armayana AhmadDocumento10 páginasEpidural Hematoma: Kurniasari Armayana AhmadSuci AlimaAinda não há avaliações
- 2005 Pedi Regional - HandoutDocumento44 páginas2005 Pedi Regional - HandoutSandhi Prabowo100% (1)
- DopamineDocumento9 páginasDopamineBaby Lyn Ann TanalgoAinda não há avaliações
- InhalDocumento33 páginasInhallupeAinda não há avaliações
- Anaesthetic Challenges and Management of Myelomeningocele RepairDocumento6 páginasAnaesthetic Challenges and Management of Myelomeningocele RepairprastiaAinda não há avaliações
- Fat Embolism Syndrome and Fractures Stabilization and Fractures StabilizationDocumento28 páginasFat Embolism Syndrome and Fractures Stabilization and Fractures StabilizationHussein HowariAinda não há avaliações
- Hassan Tonic - Clonic SeizureDocumento12 páginasHassan Tonic - Clonic SeizureHassan.shehri100% (1)
- Chronic Addiction To Dextromethorphan Cough Syrup: A Case ReportDocumento4 páginasChronic Addiction To Dextromethorphan Cough Syrup: A Case ReportEgy Saputra JayaAinda não há avaliações
- The Anatomy Physiology PainDocumento5 páginasThe Anatomy Physiology PaincrownesyaAinda não há avaliações
- Patient Controlled AnalgesiaDocumento35 páginasPatient Controlled AnalgesiamochkurniawanAinda não há avaliações
- Secondary Arterial HypertensionDocumento32 páginasSecondary Arterial HypertensionAndi SusiloAinda não há avaliações
- Inhalational Anaesthesia Mesi IDocumento84 páginasInhalational Anaesthesia Mesi IBiserat GetnetAinda não há avaliações
- Types of AnesthesiaDocumento8 páginasTypes of AnesthesiaAshlene Kate BagsiyaoAinda não há avaliações
- Chronic Pain - HO Lecture ShortDocumento28 páginasChronic Pain - HO Lecture Shortrajvikram87Ainda não há avaliações
- Bronchial AsthmaDocumento25 páginasBronchial AsthmaKamil HannaAinda não há avaliações
- Naaz 2014Documento5 páginasNaaz 2014snookumsnjAinda não há avaliações
- Types of Drugs and Its Effect On Human BodyDocumento3 páginasTypes of Drugs and Its Effect On Human Bodyshuha kamalAinda não há avaliações
- List of Substandard Drugs2006Documento8 páginasList of Substandard Drugs2006Mohammad Shahbaz AlamAinda não há avaliações
- 4 Drugs Used in GastrointestinalDocumento13 páginas4 Drugs Used in Gastrointestinalrajkumar871992Ainda não há avaliações
- 09 List & Harga 270923Documento98 páginas09 List & Harga 270923DedenAinda não há avaliações
- جداول السلائف الكيميائية 23-9-2021Documento28 páginasجداول السلائف الكيميائية 23-9-2021EmadAinda não há avaliações
- Ali Raza Pharma NotesDocumento110 páginasAli Raza Pharma NotesMuhammad Talha100% (1)
- Mechanism of Drug Action PDFDocumento1 páginaMechanism of Drug Action PDFraviomjAinda não há avaliações
- Bromo-DragonFLY ENDocumento10 páginasBromo-DragonFLY ENMarcAinda não há avaliações
- CNS Drug StudyDocumento4 páginasCNS Drug StudyMAHUSAY JOYCE CARINAAinda não há avaliações
- Formulation Development and Evaluation of Sustained Release Tablet Chlorpromazine HCLDocumento7 páginasFormulation Development and Evaluation of Sustained Release Tablet Chlorpromazine HCLWJPSR JournalAinda não há avaliações
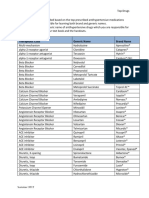
- Top Antihypertensive Drugs Generic-Brand Names PDFDocumento1 páginaTop Antihypertensive Drugs Generic-Brand Names PDFvidbala0% (1)
- Company Profile Incepta PharmaDocumento9 páginasCompany Profile Incepta PharmaNobo AhmedAinda não há avaliações
- InjectionsDocumento26 páginasInjectionsNotInterested100% (3)
- Step 1 Physiology Flash CardsDocumento22 páginasStep 1 Physiology Flash CardsbobiomeAinda não há avaliações
- D5050Documento2 páginasD5050Emilie Jane Canilang100% (2)
- 21 Susar Rev2 2006 04 11Documento26 páginas21 Susar Rev2 2006 04 11chris2272Ainda não há avaliações
- Research Concept NoteDocumento5 páginasResearch Concept NoteAbay TekalgneAinda não há avaliações
- Lecture 1 Principlesof ToxicologyDocumento16 páginasLecture 1 Principlesof ToxicologyMayuri MoreAinda não há avaliações
- Mcneil Consumer Healthcare CompanyDocumento6 páginasMcneil Consumer Healthcare CompanyJennifer JohnsonAinda não há avaliações
- Medsurg Nursing Medications Cheat Sheet: by ViaDocumento2 páginasMedsurg Nursing Medications Cheat Sheet: by ViaABEGAIL SARASUAAinda não há avaliações
- Drug Study CardinalDocumento21 páginasDrug Study CardinalDrei LanuzoAinda não há avaliações
- Name of Drug Classification Mechanism of Action Indication Contraindication Adverse Effect Nursing Consideration Generic Name: HematologicDocumento2 páginasName of Drug Classification Mechanism of Action Indication Contraindication Adverse Effect Nursing Consideration Generic Name: HematologicEsmareldah Henry SirueAinda não há avaliações
- DrugsDocumento155 páginasDrugsAkankshaAinda não há avaliações
- Nejmc 0909586Documento4 páginasNejmc 0909586theboy14juneAinda não há avaliações
- PT - Kinarya Semesta GemilangDocumento27 páginasPT - Kinarya Semesta GemilangAiko Cheryl SalsabilaAinda não há avaliações
- Pricelist Februari 2023abDocumento13 páginasPricelist Februari 2023abIka WahyuningsihAinda não há avaliações
- EpitensDocumento2 páginasEpitensmahgadAinda não há avaliações
- Toxi-Lab: The Changing Colors of Drug IdentificationDocumento8 páginasToxi-Lab: The Changing Colors of Drug IdentificationyasakbibtarlaAinda não há avaliações
- Part No Product Name Location Batch No Expired Date QTY OnhandDocumento6 páginasPart No Product Name Location Batch No Expired Date QTY OnhandRatih SafrianiAinda não há avaliações
- 3C HOSPLAB M3 Check in Activity 2 Group 5Documento22 páginas3C HOSPLAB M3 Check in Activity 2 Group 5Karren ReyesAinda não há avaliações