Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Per-Olov Kindgren - You 39 LL Never Know How Much I Loved YouDocumento5 páginasPer-Olov Kindgren - You 39 LL Never Know How Much I Loved You王建国Ainda não há avaliações
- New Second Amendment LawsuitDocumento627 páginasNew Second Amendment Lawsuitapi-3848844100% (1)
- Reading ComprehensionDocumento6 páginasReading ComprehensionvojaradAinda não há avaliações
- LAW400 Constitutional Law Winter CANDocumento99 páginasLAW400 Constitutional Law Winter CANtorcal123Ainda não há avaliações
- 2021 - Teaching Human Rights in MyanmarDocumento29 páginas2021 - Teaching Human Rights in MyanmarDuanghathai BuranajaroenkijAinda não há avaliações
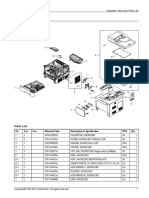
- Samsung SL-M4580FX Parts ManualDocumento27 páginasSamsung SL-M4580FX Parts Manualbill3759100% (5)
- Prevention of Sexual Harassment PolicyDocumento6 páginasPrevention of Sexual Harassment PolicyVenkatesh RYAinda não há avaliações
- Human Rights Project - Prabjot KaurDocumento14 páginasHuman Rights Project - Prabjot Kaurpraboooo100% (1)
- Comparative Policing Chapter 1 - Part 3Documento5 páginasComparative Policing Chapter 1 - Part 3Magr EscaAinda não há avaliações
- Basis of Claims and Background Information On LGBT Asylum-Seekers and Refugees From BelarusDocumento13 páginasBasis of Claims and Background Information On LGBT Asylum-Seekers and Refugees From BelarusLGBT Asylum NewsAinda não há avaliações
- Gender Midterm IIDocumento2 páginasGender Midterm IIKee Jeon DomingoAinda não há avaliações
- F2867889-67A7-4BA9-9F41-8B9C11F1D730 (2)Documento1 páginaF2867889-67A7-4BA9-9F41-8B9C11F1D730 (2)Felipe AmorosoAinda não há avaliações
- Facts of The Case (Nirbhaya Case Study)Documento6 páginasFacts of The Case (Nirbhaya Case Study)Aishwarya JadavAinda não há avaliações
- One Child Policy Powerpoint 1204636895241221 3Documento19 páginasOne Child Policy Powerpoint 1204636895241221 3Tinx LenaAinda não há avaliações
- El Cerebro y La Conducta Cap 3Documento14 páginasEl Cerebro y La Conducta Cap 3ChapaliAinda não há avaliações
- Uwi - Foun1101 - Caribbean Civilization - Topic 2Documento7 páginasUwi - Foun1101 - Caribbean Civilization - Topic 2payel02000Ainda não há avaliações
- He 9780198767237 Chapter 20Documento21 páginasHe 9780198767237 Chapter 20jaiahuja381Ainda não há avaliações
- Stop Ejk and Value Human DignityDocumento2 páginasStop Ejk and Value Human DignityQueen GAinda não há avaliações
- European Prison RulesDocumento2 páginasEuropean Prison RulesCouncil of EuropeAinda não há avaliações
- Final Project of Ipc 8TH SemDocumento17 páginasFinal Project of Ipc 8TH SemDivya RathoreAinda não há avaliações
- बाल बिबाह बिरुद्ध को रणनीति,२०७२ - 0Documento18 páginasबाल बिबाह बिरुद्ध को रणनीति,२०७२ - 0siddharthalaw123Ainda não há avaliações
- Uncrc AdhdDocumento20 páginasUncrc AdhdKelley Dobson-SmithAinda não há avaliações
- Saplad Vawc ReportsDocumento7 páginasSaplad Vawc ReportsbarangaysapladAinda não há avaliações
- Deche - Legal Responses To Intra-Familial Child Sexual Abuse in Kenya - A Case For Restorative JusticeDocumento252 páginasDeche - Legal Responses To Intra-Familial Child Sexual Abuse in Kenya - A Case For Restorative JusticeKisumbaAinda não há avaliações
- H-ATCM (2003) 001 enDocumento118 páginasH-ATCM (2003) 001 enpiotr_korzec3475Ainda não há avaliações
- مكتبة نور التشيؤ أكسل هونيث ترجمة بومنير 2 PDFDocumento125 páginasمكتبة نور التشيؤ أكسل هونيث ترجمة بومنير 2 PDFصالح محفوظيAinda não há avaliações
- PDF Torture in Healthcare Publication PDFDocumento346 páginasPDF Torture in Healthcare Publication PDFsanjnuAinda não há avaliações
- Las Negociaciones en El Mundo 3 T Cticas de Las Negociaciones Internacionales PDFDocumento30 páginasLas Negociaciones en El Mundo 3 T Cticas de Las Negociaciones Internacionales PDFRossanaGR0% (1)
- "Chapter 2: Rights in The Indian Constitution ": F R I CDocumento4 páginas"Chapter 2: Rights in The Indian Constitution ": F R I Craj pandeyAinda não há avaliações
- LSM Case Note 2021Documento5 páginasLSM Case Note 2021Miral HasanAinda não há avaliações