Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Women in Politics 2015Documento1 páginaWomen in Politics 2015Inter-Parliamentary Union100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- AVAC AIDS Tipping PointDocumento1 páginaAVAC AIDS Tipping PointmurphmanAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Women Deliver 2013 Webcast ScheduleDocumento6 páginasWomen Deliver 2013 Webcast SchedulemurphmanAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- WFP 229327Documento1 páginaWFP 229327murphmanAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- PSI 2012 ImpactDocumento1 páginaPSI 2012 ImpactmurphmanAinda não há avaliações
- Pneumonia InfographicDocumento1 páginaPneumonia InfographicmurphmanAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Lough Erne DeclarationDocumento1 páginaLough Erne DeclarationTelegraphUKAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- WCD Infographic Know Your OptionsDocumento1 páginaWCD Infographic Know Your OptionsmurphmanAinda não há avaliações
- How Much of Your U.S. Taxes Goes Toward Stopping AIDS, Malaria and Child Mortality?Documento1 páginaHow Much of Your U.S. Taxes Goes Toward Stopping AIDS, Malaria and Child Mortality?murphmanAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- USGLC RoadmapDocumento1 páginaUSGLC RoadmapmurphmanAinda não há avaliações
- International Development in The Blogosphere: Ryann ManningDocumento37 páginasInternational Development in The Blogosphere: Ryann ManningmurphmanAinda não há avaliações
- ER App Deadliest Dis InfoDocumento1 páginaER App Deadliest Dis InfomurphmanAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Map 3010Documento1 páginaMap 3010murphmanAinda não há avaliações
- Infograph Everyday UN BwcunaDocumento2 páginasInfograph Everyday UN BwcunamurphmanAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Different Schools of Development Thought and Beliefs About LeadershipDocumento2 páginasDifferent Schools of Development Thought and Beliefs About LeadershipmurphmanAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- 12 0196 Polis Report Inner v12Documento24 páginas12 0196 Polis Report Inner v12murphmanAinda não há avaliações
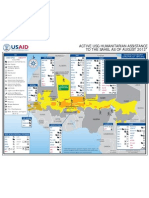
- 08.31.12 - USAID-DCHA Sahel Food Insecurity and Complex Emergency Program Map #15Documento1 página08.31.12 - USAID-DCHA Sahel Food Insecurity and Complex Emergency Program Map #15murphmanAinda não há avaliações
- Prev Spotlight Condoms FinalDocumento8 páginasPrev Spotlight Condoms FinalmurphmanAinda não há avaliações
- 08.31.12 - USAID-DCHA Sahel Food Insecurity and Complex Emergency Program Map #15Documento1 página08.31.12 - USAID-DCHA Sahel Food Insecurity and Complex Emergency Program Map #15murphmanAinda não há avaliações
- Worldwide HumanitarianAidWorkers 2012aug15 HIU U618Documento1 páginaWorldwide HumanitarianAidWorkers 2012aug15 HIU U618markleongoldber3215Ainda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- OCHA Funding in SudanDocumento1 páginaOCHA Funding in SudanmurphmanAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- Sudan Bombing Info GraphicDocumento1 páginaSudan Bombing Info GraphicmurphmanAinda não há avaliações
- Mobile Info Graphic Uganda Kenyan EquivalentDocumento1 páginaMobile Info Graphic Uganda Kenyan EquivalentmurphmanAinda não há avaliações
- Beyondkony2012 SampleDocumento18 páginasBeyondkony2012 SamplemurphmanAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- CHMI Report 112711 High LinksDocumento32 páginasCHMI Report 112711 High LinksmurphmanAinda não há avaliações
- The Changing Face of AIDSDocumento1 páginaThe Changing Face of AIDSmurphmanAinda não há avaliações
- Developing Influence ADocumento1 páginaDeveloping Influence AmurphmanAinda não há avaliações
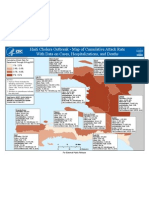
- HA Cholera MSPP Data Population Cases Attack Rate CDC-SA-GRASP (02-Sep-2011)Documento1 páginaHA Cholera MSPP Data Population Cases Attack Rate CDC-SA-GRASP (02-Sep-2011)murphmanAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Mo Ibrahim Index 2011Documento1 páginaMo Ibrahim Index 2011murphmanAinda não há avaliações
- Male Multiple Orgasm SurveyDocumento3 páginasMale Multiple Orgasm SurveygmeadesAinda não há avaliações
- The Porn Circuit Ebook Prov423Documento47 páginasThe Porn Circuit Ebook Prov423sherm77100% (1)
- GuideDocumento150 páginasGuideavulkAinda não há avaliações
- IASR Policy BriefDocumento12 páginasIASR Policy BriefJaphet Grace MoletaAinda não há avaliações
- Cultural Studies AssignmentDocumento3 páginasCultural Studies AssignmentSaif Ali AhmadAinda não há avaliações
- Submissive ProtocolDocumento12 páginasSubmissive ProtocolKing Karvo89% (71)
- Voices From The Margins - Street Children's Subcultures in IndonesiaDocumento21 páginasVoices From The Margins - Street Children's Subcultures in IndonesialindaokeeffeAinda não há avaliações
- Sexual Healing Pamphlet 2009Documento6 páginasSexual Healing Pamphlet 2009Ganesh PrasadAinda não há avaliações
- Homosexuality: A History (From Ancient Greece To Gay Liberation) Vern L. BulloughDocumento209 páginasHomosexuality: A History (From Ancient Greece To Gay Liberation) Vern L. BulloughhugopraisAinda não há avaliações
- Predictors of Relationship Satisfaction in BDSM RelationshipsDocumento58 páginasPredictors of Relationship Satisfaction in BDSM RelationshipsYvonne Yap Ying YingAinda não há avaliações
- Understanding Sexuality, Love and RelationshipsDocumento32 páginasUnderstanding Sexuality, Love and RelationshipsMariaLea Serrano AlmosuraAinda não há avaliações
- Speech On ProstitutionDocumento3 páginasSpeech On Prostitutionappyhamid100% (5)
- Anthropology Rediscovers Sexuality-A Theoretical Comment PDFDocumento10 páginasAnthropology Rediscovers Sexuality-A Theoretical Comment PDFHeyy8Ainda não há avaliações
- NakshtraDocumento2 páginasNakshtraChandra PoojariAinda não há avaliações
- Sexual OffencesDocumento56 páginasSexual Offenceswrashwan27Ainda não há avaliações
- NYC Bathhouse Battles of 1985: Sex, Politics and AIDSDocumento108 páginasNYC Bathhouse Battles of 1985: Sex, Politics and AIDSAramael Andres Pena-AlcantaraAinda não há avaliações
- 21 Hypersexual in Dementia PDFDocumento6 páginas21 Hypersexual in Dementia PDFSusi RutmalemAinda não há avaliações
- Position Paper: (In Favor of Censorship in Filipino Movies)Documento3 páginasPosition Paper: (In Favor of Censorship in Filipino Movies)Ysabelle PazAinda não há avaliações
- Human Sexuality NodrmDocumento597 páginasHuman Sexuality Nodrmshaahin13631363Ainda não há avaliações
- 3X MethodDocumento13 páginas3X MethodNobodyAinda não há avaliações
- Child Marriage and HIV in Rural IndiaDocumento13 páginasChild Marriage and HIV in Rural IndiaArjinder SinghAinda não há avaliações
- For Sale: Mark AguharDocumento47 páginasFor Sale: Mark Aguharmaguhar7728Ainda não há avaliações
- INFOSEM Final ReportDocumento40 páginasINFOSEM Final ReportManasa BanothAinda não há avaliações
- Treatment of Sex Addiction: Goals and ObjectivesDocumento2 páginasTreatment of Sex Addiction: Goals and ObjectivesDorothy Hayden100% (1)
- Money J. Two Cases of Amptutation As A ParaphiliaDocumento12 páginasMoney J. Two Cases of Amptutation As A ParaphiliaROGELIO VAZQUEZ RAMIREZAinda não há avaliações
- Adolescent Counselling ChoDocumento37 páginasAdolescent Counselling ChoShankar Murari100% (1)
- Khwaja Sara: "Transgender" Activism and Transnationality in Pakistan (Faris A. Khan)Documento16 páginasKhwaja Sara: "Transgender" Activism and Transnationality in Pakistan (Faris A. Khan)Faris A. KhanAinda não há avaliações
- Full Download The Adolescent Development Relationships and Culture 14th Edition Ebook PDFDocumento42 páginasFull Download The Adolescent Development Relationships and Culture 14th Edition Ebook PDFbarbara.coakley466100% (33)
- Premarital SexDocumento24 páginasPremarital SexHafizatulSalmaAinda não há avaliações
- How Sleazy Are YouDocumento3 páginasHow Sleazy Are Youapi-3696324100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (13)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 3.5 de 5 estrelas3.5/5 (2)
- The Wicked and the Willing: An F/F Gothic Horror Vampire NovelNo EverandThe Wicked and the Willing: An F/F Gothic Horror Vampire NovelNota: 4 de 5 estrelas4/5 (20)
- Prisoners of Geography: Ten Maps That Explain Everything About the WorldNo EverandPrisoners of Geography: Ten Maps That Explain Everything About the WorldNota: 4.5 de 5 estrelas4.5/5 (1143)
- Selling the Dream: The Billion-Dollar Industry Bankrupting AmericansNo EverandSelling the Dream: The Billion-Dollar Industry Bankrupting AmericansNota: 4 de 5 estrelas4/5 (17)