Você também pode gostar
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Naspub KEGIATAN ELEKTIFDocumento11 páginasNaspub KEGIATAN ELEKTIFImam HartonoAinda não há avaliações
- Copy JurnalDocumento6 páginasCopy JurnalImam HartonoAinda não há avaliações
- Paediatrica Indonesiana: Harris Alfan, Rita Dewi Arifin, Erial Bahar, Syarif Darwin AnsoriDocumento6 páginasPaediatrica Indonesiana: Harris Alfan, Rita Dewi Arifin, Erial Bahar, Syarif Darwin AnsoriImam HartonoAinda não há avaliações
- Effect of Mass Supplementation With Ready-to-Use Supplementary Food During An Anticipated Nutritional EmergencyDocumento8 páginasEffect of Mass Supplementation With Ready-to-Use Supplementary Food During An Anticipated Nutritional EmergencyImam HartonoAinda não há avaliações
- KatarakDocumento27 páginasKatarakImam HartonoAinda não há avaliações
- Cost-Effectiveness of Community-Based Treatment of Severe Acute Malnutrition in ChildrenDocumento8 páginasCost-Effectiveness of Community-Based Treatment of Severe Acute Malnutrition in ChildrenImam HartonoAinda não há avaliações
- Risk Factors For Childhood Malnutrition in Roma Settlements in SerbiaDocumento8 páginasRisk Factors For Childhood Malnutrition in Roma Settlements in SerbiaImam HartonoAinda não há avaliações
- Lipolysis LipogenesisDocumento11 páginasLipolysis LipogenesisImam HartonoAinda não há avaliações
- Ajph 51 1 106Documento2 páginasAjph 51 1 106Imam HartonoAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Reference 2Documento4 páginasReference 2Tari De ArimbieAinda não há avaliações
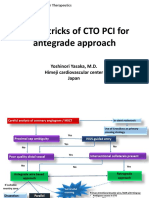
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocumento21 páginasTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureAinda não há avaliações
- Jessica Newton Imaging Technologies February 2, 2011Documento3 páginasJessica Newton Imaging Technologies February 2, 2011jnewton4Ainda não há avaliações
- Guyton at The BedsideDocumento7 páginasGuyton at The BedsideGustavo ParedesAinda não há avaliações
- PHCP FinalsDocumento75 páginasPHCP FinalsSamantha SantosAinda não há avaliações
- Cardiac surgery 5th year 2017-محلولDocumento11 páginasCardiac surgery 5th year 2017-محلولIbrahim BarhamAinda não há avaliações
- Amiodarone and Lidocaine For The Treatment 1 1Documento11 páginasAmiodarone and Lidocaine For The Treatment 1 1vanniAinda não há avaliações
- Coronary Atery Disease-Htn-Thrombo QuestionsDocumento38 páginasCoronary Atery Disease-Htn-Thrombo Questionssrivari sriniAinda não há avaliações
- Indikasi TrombektomiDocumento6 páginasIndikasi TrombektomiNatasha BastiaanAinda não há avaliações
- Atrioventricular Septal DefectDocumento3 páginasAtrioventricular Septal DefectManishta Menaka DhuromsinghAinda não há avaliações
- NUR3111 Nursing Care Plan Copy 1Documento19 páginasNUR3111 Nursing Care Plan Copy 1liAinda não há avaliações
- Detailed Lesson Plan in Science 5 1st QuarterDocumento8 páginasDetailed Lesson Plan in Science 5 1st QuarterAndrewAinda não há avaliações
- J Strength Cond Res - 2011 - A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionDocumento8 páginasJ Strength Cond Res - 2011 - A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionTAINAH DE PAULAAinda não há avaliações
- Physiology-Summary NotesDocumento201 páginasPhysiology-Summary NotesReem NasserAinda não há avaliações
- Innovations in Cardiovascular Disease ManagementDocumento183 páginasInnovations in Cardiovascular Disease ManagementGopal Kumar DasAinda não há avaliações
- Antiplatelet and Thrombolytic DrugsDocumento48 páginasAntiplatelet and Thrombolytic DrugsNofa PuspitaAinda não há avaliações
- Precourse Self-Assessment ResultsDocumento3 páginasPrecourse Self-Assessment ResultsDioseptyaAinda não há avaliações
- Chapter 23: Drugs Used To Treat HypertensionDocumento14 páginasChapter 23: Drugs Used To Treat HypertensionAziil LiizaAinda não há avaliações
- Accelerated Idioventricular RhythmDocumento5 páginasAccelerated Idioventricular RhythmMed AmineAinda não há avaliações
- Jadwal Sympo Edit1Documento3 páginasJadwal Sympo Edit1reyAinda não há avaliações
- Arteriovenous Hemangioma, M 45, BackDocumento5 páginasArteriovenous Hemangioma, M 45, BackDeba P SarmaAinda não há avaliações
- Emergency MedicineDocumento150 páginasEmergency MedicineDev MartelAinda não há avaliações
- ECG Changes in Drug and Electrolyte AbnormalitiesDocumento28 páginasECG Changes in Drug and Electrolyte AbnormalitiesNachiket Vijay PotdarAinda não há avaliações
- ACLS Algorithms SlideDocumento26 páginasACLS Algorithms SlidehrsoAinda não há avaliações
- CCrISP 7 Shock and HaemorrhageDocumento27 páginasCCrISP 7 Shock and HaemorrhageDrSayk YousufAinda não há avaliações
- Pulmonary EdemaDocumento32 páginasPulmonary EdemaAshraf Jonidee100% (1)
- Heart Sound & MurmursDocumento11 páginasHeart Sound & MurmursTraceyAinda não há avaliações
- Vessel Wall 1Documento12 páginasVessel Wall 1Matheus Nucci RiccettoAinda não há avaliações
- VT Vs SVT WellensDocumento8 páginasVT Vs SVT WellensLucas KruschevAinda não há avaliações
- Imaging of Cardiac TraumaDocumento14 páginasImaging of Cardiac TraumaAlejandro ColombanoAinda não há avaliações