Você também pode gostar
- Self-Medication (PSBH Project 2010)Documento54 páginasSelf-Medication (PSBH Project 2010)Varun Shah100% (1)
- Routes of Drug EliminationDocumento17 páginasRoutes of Drug EliminationdahiphalehAinda não há avaliações
- Drug InteractionDocumento27 páginasDrug InteractionRida Nur RafidahAinda não há avaliações
- Physicochemical IncompatibilitiesDocumento20 páginasPhysicochemical Incompatibilitiesvicbart11Ainda não há avaliações
- Absorption of DrugsDocumento24 páginasAbsorption of DrugsShrikant SharmaAinda não há avaliações
- Principles of Pharmacology Chapter 1Documento37 páginasPrinciples of Pharmacology Chapter 1Muhammad ZakriaAinda não há avaliações
- Loshieni Shri - Drug Product PerformanceDocumento10 páginasLoshieni Shri - Drug Product PerformanceloshieniAinda não há avaliações
- Ch4 Cost-Minimization Analysis PDFDocumento12 páginasCh4 Cost-Minimization Analysis PDFAhmad Makhlouf100% (1)
- 4-Drug Delivery Systems (Autosaved)Documento41 páginas4-Drug Delivery Systems (Autosaved)Chelle PaloAinda não há avaliações
- Drugs Interaction1Documento13 páginasDrugs Interaction1Akshay MandhotraAinda não há avaliações
- Factors Influencing Drug Absorption Though Git PDFDocumento59 páginasFactors Influencing Drug Absorption Though Git PDFRamakant JoshiAinda não há avaliações
- Therapeutic Drug Monitoring 7-1-20Documento27 páginasTherapeutic Drug Monitoring 7-1-20mofadhilAinda não há avaliações
- Paracetamol Literature - Navneet BaggaDocumento21 páginasParacetamol Literature - Navneet BaggaNAVNEET BAGGAAinda não há avaliações
- 11 PD Drug Interaction EngDocumento14 páginas11 PD Drug Interaction EngshahrukhziaAinda não há avaliações
- Understanding PharmacologyDocumento57 páginasUnderstanding Pharmacologyarun231187Ainda não há avaliações
- AtropineDocumento14 páginasAtropineKrazygopa BalorAinda não há avaliações
- Statement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistDocumento5 páginasStatement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistAprilia R. Permatasari0% (1)
- Biotransformation of DrugsDocumento22 páginasBiotransformation of DrugsZaigham Hammad100% (1)
- Drug - Excipient InteractionsDocumento32 páginasDrug - Excipient InteractionsNoor hossain100% (1)
- Group 5 Pdis211 Lab E1Documento22 páginasGroup 5 Pdis211 Lab E1Mikaela Kean JoseAinda não há avaliações
- Drug InteractionDocumento20 páginasDrug InteractionRajendra Moorthy RajendranAinda não há avaliações
- Pharmacokinetics and Pharmacodynamics 40Documento40 páginasPharmacokinetics and Pharmacodynamics 40Shoaib BiradarAinda não há avaliações
- Clinical Pharmacokinetics and Pharmacodynamics: Dr. Abaasi KabogoDocumento52 páginasClinical Pharmacokinetics and Pharmacodynamics: Dr. Abaasi KabogoNina100% (1)
- Effervescent GranulesDocumento6 páginasEffervescent GranulesVarinder KumarAinda não há avaliações
- Autacoid PharmacologyDocumento38 páginasAutacoid PharmacologyAakkkAinda não há avaliações
- MothballsDocumento2 páginasMothballsReg ArbotanteAinda não há avaliações
- Receptors As Drug Targets PDFDocumento66 páginasReceptors As Drug Targets PDFAubreyAinda não há avaliações
- Beer Lambert LawDocumento3 páginasBeer Lambert LawRobert Ribeiro100% (2)
- 1 Herbs and Health ProductsDocumento29 páginas1 Herbs and Health ProductsanavyaledzurcAinda não há avaliações
- Laboratory Manual Pharmaceutics Ii Laboratory Manual Cum Logbook 3 1 2 - PHT Level VDocumento66 páginasLaboratory Manual Pharmaceutics Ii Laboratory Manual Cum Logbook 3 1 2 - PHT Level VTIVIYAH THEVAR 1017Ainda não há avaliações
- Pharm 231: Hospital Pharmacy: Iii. Medication ProfileDocumento3 páginasPharm 231: Hospital Pharmacy: Iii. Medication ProfileTESORO Zeus DavidAinda não há avaliações
- Screening and Pharmacy 2019 - TM02Documento48 páginasScreening and Pharmacy 2019 - TM02A'Ilda MAinda não há avaliações
- 6 Pharmacists in Public HealthDocumento22 páginas6 Pharmacists in Public HealthJoanna Carla Marmonejo Estorninos-Walker100% (1)
- ProdrugsDocumento23 páginasProdrugsMankaran SinghAinda não há avaliações
- DPCODocumento30 páginasDPCOArya SreedharanAinda não há avaliações
- Drug Discovery and Development: From Bench to BedsideDocumento23 páginasDrug Discovery and Development: From Bench to BedsideAhmed HamarnehAinda não há avaliações
- Incompatibility IV AdmixtureDocumento17 páginasIncompatibility IV AdmixtureClara Herlina100% (1)
- 3B - Clinical PharmacyDocumento35 páginas3B - Clinical PharmacyekramAinda não há avaliações
- Chapter 9: Solid Oral Modified-Release Dosage Forms and Drug Delivery SystemsDocumento26 páginasChapter 9: Solid Oral Modified-Release Dosage Forms and Drug Delivery SystemsAlecza Mae Savella100% (1)
- Ward Round Participation Benefits for PharmacistsDocumento2 páginasWard Round Participation Benefits for PharmacistsAnonymous whcvnPBeQAinda não há avaliações
- IncompatibilityDocumento4 páginasIncompatibilityNaresh YechuriAinda não há avaliações
- TransfersomesDocumento33 páginasTransfersomesRajesh Thipparaboina50% (2)
- Introduction To Pharmacoepidemiology 2015 PDFDocumento20 páginasIntroduction To Pharmacoepidemiology 2015 PDFNovria Rizki HarahapAinda não há avaliações
- LiberationDocumento33 páginasLiberationAnthony Catapang PascualAinda não há avaliações
- Flavanoids, L 3Documento48 páginasFlavanoids, L 3Ammadazfar ImamAinda não há avaliações
- Factors Influencing Bioavailability of Drugs PDFDocumento2 páginasFactors Influencing Bioavailability of Drugs PDFRoy50% (2)
- Module 3: Hospital Pharmacy: Prepared By: Alexandra D. Atienza RPHDocumento135 páginasModule 3: Hospital Pharmacy: Prepared By: Alexandra D. Atienza RPHJojo DelosreyesAinda não há avaliações
- Colon Drug Delivery System: BY, Keerthivardhan.D M-Pharm 2 SemesterDocumento26 páginasColon Drug Delivery System: BY, Keerthivardhan.D M-Pharm 2 SemesterDian AvicennaAinda não há avaliações
- Controls: I. Material ControlDocumento11 páginasControls: I. Material ControlDaena TimtimanAinda não há avaliações
- Cardiovascular System: Antihypertensive DrugsDocumento73 páginasCardiovascular System: Antihypertensive Drugsأمجد محمدAinda não há avaliações
- Extended Release Drug Delivery ReviewDocumento9 páginasExtended Release Drug Delivery ReviewTuyến Đặng ThịAinda não há avaliações
- Autacoids: Histamine, Kinins, Serotonin and OndansetronDocumento43 páginasAutacoids: Histamine, Kinins, Serotonin and OndansetronOdiete EfeAinda não há avaliações
- Kinetics of DrugsDocumento18 páginasKinetics of DrugsAnne DeeAinda não há avaliações
- Social and Administrative PharmacyDocumento18 páginasSocial and Administrative PharmacyMarianne Cruz100% (1)
- BIOAVAILABILITY AND BIOEQUIVALANCE STUDIES Final - PPTX'Documento32 páginasBIOAVAILABILITY AND BIOEQUIVALANCE STUDIES Final - PPTX'Md TayfuzzamanAinda não há avaliações
- Immunization Policy Guidline - Kenya 2013Documento72 páginasImmunization Policy Guidline - Kenya 2013okwadha simionAinda não há avaliações
- Community Pharmacy Intern Exercises5-9Documento6 páginasCommunity Pharmacy Intern Exercises5-9Joslin RozAinda não há avaliações
- ExcretionDocumento35 páginasExcretionHely PatelAinda não há avaliações
- Anup GanoreDocumento29 páginasAnup GanoreSuyesh KaleAinda não há avaliações
- A Review On Delivery of Drugs Used For Acid Reflux Treatment Using Buccal DrugDocumento18 páginasA Review On Delivery of Drugs Used For Acid Reflux Treatment Using Buccal DrugAnjali Sahil MittalAinda não há avaliações
- Taste Masked SuspensionDocumento7 páginasTaste Masked SuspensionPharmacognosy JournalAinda não há avaliações
- Resealed Erythrocytes As A Carrier For Drug TargetingDocumento9 páginasResealed Erythrocytes As A Carrier For Drug TargetingPharmacognosy JournalAinda não há avaliações
- Fast Dissolving Drug Delivery and Its TechnologiesDocumento6 páginasFast Dissolving Drug Delivery and Its TechnologiesPharmacognosy JournalAinda não há avaliações
- Role of Pharmacist Management and NovelDocumento12 páginasRole of Pharmacist Management and NovelPharmacognosy JournalAinda não há avaliações
- Formulation and Pharmacological Evaluation ofDocumento15 páginasFormulation and Pharmacological Evaluation ofPharmacognosy JournalAinda não há avaliações
- Recent Trends in Liposomes Used As Novel DrugDocumento10 páginasRecent Trends in Liposomes Used As Novel DrugPharmacognosy JournalAinda não há avaliações
- Diabetes Epidemic in IndiaDocumento17 páginasDiabetes Epidemic in IndiaPharmacognosy JournalAinda não há avaliações
- Polysaccharides and Natural Gums For Colon DrugDocumento5 páginasPolysaccharides and Natural Gums For Colon DrugPharmacognosy JournalAinda não há avaliações
- Fast Dissolving Tablet - A ReviewDocumento7 páginasFast Dissolving Tablet - A ReviewPharmacognosy JournalAinda não há avaliações
- Bio Markers Its Novel ApplicationDocumento7 páginasBio Markers Its Novel ApplicationPharmacognosy JournalAinda não há avaliações
- Glaucoma - A Eye Disorder Its Causes, Risk Factor, Prevention and MedicationDocumento16 páginasGlaucoma - A Eye Disorder Its Causes, Risk Factor, Prevention and MedicationPharmacognosy JournalAinda não há avaliações
- A Review On Oral Mucosal Drug Delivery SystemDocumento8 páginasA Review On Oral Mucosal Drug Delivery SystemPharmacognosy JournalAinda não há avaliações
- Techno - Economic Feasibility Study To Establish Gelatin & Glue Production PlantDocumento53 páginasTechno - Economic Feasibility Study To Establish Gelatin & Glue Production PlantMohammed Abbas100% (1)
- Basic Medical KnowledgeDocumento6 páginasBasic Medical Knowledgedoctor zoneAinda não há avaliações
- Dosing Disc Thickness Calculation For Capsule Filling Machine - SaintyTecDocumento4 páginasDosing Disc Thickness Calculation For Capsule Filling Machine - SaintyTecSangram KendreAinda não há avaliações
- Pharmaceutical Technology Training Manual-2fDocumento80 páginasPharmaceutical Technology Training Manual-2fJhem Martinez100% (1)
- PQA Stability TestingDocumento21 páginasPQA Stability Testingbaby shazanaAinda não há avaliações
- Report of Industrial Visit To Kopran PhaDocumento4 páginasReport of Industrial Visit To Kopran PhaManish Kushwaha05Ainda não há avaliações
- IR NishaDocumento41 páginasIR NishabpharmbaAinda não há avaliações
- Everything About DogsDocumento326 páginasEverything About Dogstobiasaxo5653100% (1)
- DDS-lab Midterm ReviewerDocumento13 páginasDDS-lab Midterm Reviewerchincaluscusin4Ainda não há avaliações
- Introduction To Pharmaceutics - Dosage FormsDocumento70 páginasIntroduction To Pharmaceutics - Dosage FormsJuvelyn Kyle GugmaAinda não há avaliações
- 11health - EnglishDocumento42 páginas11health - Englishkolipaka rajeshAinda não há avaliações
- 1.1 Pharmaceutics - I: (B) Introduction To Ayurvedic Dosage FormsDocumento19 páginas1.1 Pharmaceutics - I: (B) Introduction To Ayurvedic Dosage FormsAteeque AnsariAinda não há avaliações
- Impact of Business Level StrategiesDocumento10 páginasImpact of Business Level StrategiesnayontaniaAinda não há avaliações
- Gastroretentive Drug Delivery System (GRDDS)Documento32 páginasGastroretentive Drug Delivery System (GRDDS)Hely PatelAinda não há avaliações
- Hard Gelatin Capsules Today and TomorrowDocumento23 páginasHard Gelatin Capsules Today and TomorrowCarlos CantilloAinda não há avaliações
- Bank AsiaDocumento85 páginasBank AsiajehanAinda não há avaliações
- Administration of Medicines To Adult Patients Who Cannot Swallow Tablets or Capsules UHL GuidelineDocumento10 páginasAdministration of Medicines To Adult Patients Who Cannot Swallow Tablets or Capsules UHL GuidelineFabiola NogaAinda não há avaliações
- Unit-Iii CapsulesDocumento88 páginasUnit-Iii Capsulesteenu josenAinda não há avaliações
- Manufacturing Units Having Who GMP CertificationDocumento34 páginasManufacturing Units Having Who GMP Certificationchirag100% (2)
- Capsules - Remington - The Science and Practice of PharmacyDocumento8 páginasCapsules - Remington - The Science and Practice of Pharmacyjuananzaldo266Ainda não há avaliações
- Vivapur MCC Spheres GB 1009Documento4 páginasVivapur MCC Spheres GB 1009drantistAinda não há avaliações
- Ag Listing 04jan2024Documento97 páginasAg Listing 04jan2024monkeAinda não há avaliações
- Crosslinking Studies in Gelatin Capsules Treated With Formaldehyde and in Capsules Exposed To Elevated Temperature and HumidityDocumento10 páginasCrosslinking Studies in Gelatin Capsules Treated With Formaldehyde and in Capsules Exposed To Elevated Temperature and HumidityLaura ZuletaAinda não há avaliações
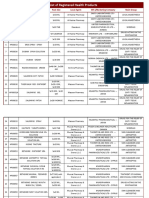
- EGYPT Registered Products Update 22-10-09 1Documento103 páginasEGYPT Registered Products Update 22-10-09 1Anuj MairhAinda não há avaliações
- Shin, Seol, Son - Interpretation of Animal Dose and Human Equivalent Dose For Drug Development - 2010 PDFDocumento7 páginasShin, Seol, Son - Interpretation of Animal Dose and Human Equivalent Dose For Drug Development - 2010 PDFHendra Wana Nur'aminAinda não há avaliações
- Pharmaceutical Dosage FormsDocumento52 páginasPharmaceutical Dosage Formsapi-3750955100% (5)
- MPH FridayDocumento7 páginasMPH FridayPsAb HSAinda não há avaliações
- Particle Size of Granules and Mechanical Properties of Paracetamol TabletsDocumento3 páginasParticle Size of Granules and Mechanical Properties of Paracetamol TabletsAdnanAinda não há avaliações
- Caplin Point PDFDocumento257 páginasCaplin Point PDFkailasAinda não há avaliações
- Pharmacy Paper I & II TopicsDocumento2 páginasPharmacy Paper I & II TopicsShadman RhamanAinda não há avaliações