Você também pode gostar
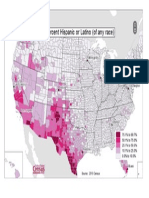
- US Map of Hispanic Population by CountyDocumento1 páginaUS Map of Hispanic Population by CountyGeneric_PersonaAinda não há avaliações
- Crown & Baptist Streets Village Group: ST Re EtDocumento1 páginaCrown & Baptist Streets Village Group: ST Re EtGeneric_PersonaAinda não há avaliações
- Peach Leaf CurlDocumento3 páginasPeach Leaf CurlGeneric_PersonaAinda não há avaliações
- Sydney As A Global CityDocumento9 páginasSydney As A Global CityGeneric_PersonaAinda não há avaliações
- The Rise of The Individual in Modern ChinaDocumento3 páginasThe Rise of The Individual in Modern ChinaGeneric_PersonaAinda não há avaliações
- English Language in Hong KongDocumento13 páginasEnglish Language in Hong KongGeneric_PersonaAinda não há avaliações
- Earnings of ImmigrantsDocumento23 páginasEarnings of ImmigrantsGeneric_PersonaAinda não há avaliações
- Monument of Myth: The Basilica of Sacre CouerDocumento20 páginasMonument of Myth: The Basilica of Sacre CouerGeneric_PersonaAinda não há avaliações
- Result of Portrayals of Latinos On TVDocumento33 páginasResult of Portrayals of Latinos On TVGeneric_PersonaAinda não há avaliações
- Citizens United ReviewDocumento5 páginasCitizens United ReviewGeneric_PersonaAinda não há avaliações
- Sydney Australia's Green Sector OpportunityDocumento8 páginasSydney Australia's Green Sector OpportunityGeneric_PersonaAinda não há avaliações
- China and Sydney Australias Growing Business PartnershipDocumento8 páginasChina and Sydney Australias Growing Business PartnershipGeneric_PersonaAinda não há avaliações
- Agenda Setting, Public Opinion & Immigration ReformDocumento21 páginasAgenda Setting, Public Opinion & Immigration ReformGeneric_PersonaAinda não há avaliações
- Measuring Helix Angle of GearsDocumento6 páginasMeasuring Helix Angle of Gearsdarshan.hegdebAinda não há avaliações
- Risk-Managing Revolution (Arab Spring)Documento4 páginasRisk-Managing Revolution (Arab Spring)Generic_PersonaAinda não há avaliações
- The Diversity of Debt Crises in EuropeDocumento18 páginasThe Diversity of Debt Crises in EuropeGeneric_PersonaAinda não há avaliações
- Grizzly Hevy Duty Wood Lathe ManualDocumento60 páginasGrizzly Hevy Duty Wood Lathe ManualGeneric_PersonaAinda não há avaliações
- Educated Preferences: Explaining Attitudes Toward Immigration in EuropeDocumento44 páginasEducated Preferences: Explaining Attitudes Toward Immigration in EuropeGeneric_PersonaAinda não há avaliações
- Promoting Economic Liberalization in EgyptDocumento14 páginasPromoting Economic Liberalization in EgyptGeneric_PersonaAinda não há avaliações
- Protests in An Information SocietyDocumento25 páginasProtests in An Information SocietyGeneric_PersonaAinda não há avaliações
- A Study On The Effects of Sexually Explicit Advertisement On MemoryDocumento10 páginasA Study On The Effects of Sexually Explicit Advertisement On MemoryGeneric_PersonaAinda não há avaliações
- Empowering Youth - Technology in Advocacy To Affect Social ChangeDocumento18 páginasEmpowering Youth - Technology in Advocacy To Affect Social ChangeGeneric_PersonaAinda não há avaliações
- Internet, Mass Communication & Collective ActionDocumento12 páginasInternet, Mass Communication & Collective ActionGeneric_PersonaAinda não há avaliações
- US Policy and The International Dimensions of Failed Democratic Transitions in The Arab WorldDocumento18 páginasUS Policy and The International Dimensions of Failed Democratic Transitions in The Arab WorldGeneric_PersonaAinda não há avaliações
- The Rise of The Individual in Modern ChinaDocumento3 páginasThe Rise of The Individual in Modern ChinaGeneric_PersonaAinda não há avaliações
- Title Insert (Derogatory Words) Research StudyDocumento5 páginasTitle Insert (Derogatory Words) Research StudyGeneric_PersonaAinda não há avaliações
- English Language in Hong KongDocumento13 páginasEnglish Language in Hong KongGeneric_PersonaAinda não há avaliações
- Prilleltensky.2008.Role of Power in Wellness-Oppression-Liberation - JCP PDFDocumento21 páginasPrilleltensky.2008.Role of Power in Wellness-Oppression-Liberation - JCP PDFcastrolaAinda não há avaliações
- Aggressive Behavior Following StrokeDocumento5 páginasAggressive Behavior Following StrokeGeneric_PersonaAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Dr. Sherif Eladawy Dr. Amr Bassiouny Dr. Yehia Hussein: Presented byDocumento8 páginasDr. Sherif Eladawy Dr. Amr Bassiouny Dr. Yehia Hussein: Presented byYahya Hassan Hussein El-tamalyAinda não há avaliações
- Desfibrilador Automatico Externo Schiller Fred EasyDocumento47 páginasDesfibrilador Automatico Externo Schiller Fred EasyDuvan Morales GuzmanAinda não há avaliações
- Ventricular Arrhythmia - VT: Braghmandaru A.BDocumento113 páginasVentricular Arrhythmia - VT: Braghmandaru A.BFaisol SiddiqAinda não há avaliações
- Manoj DissertationDocumento82 páginasManoj DissertationSheela ShahAinda não há avaliações
- Critical Incident AnalysisDocumento5 páginasCritical Incident Analysiszaim tech33% (3)
- Shibly Rahman PacesDocumento356 páginasShibly Rahman PacesMohammadAbdurRahmanAinda não há avaliações
- Mishba +pharmacology + Tapan ShahDocumento232 páginasMishba +pharmacology + Tapan ShahRaushan BlakeAinda não há avaliações
- Pharmacokinetics Compartment ModelingDocumento94 páginasPharmacokinetics Compartment ModelingPinkishBlue100% (1)
- Daftar Seminar Q SIPDocumento2 páginasDaftar Seminar Q SIPririn widyaAinda não há avaliações
- Pomr 1Documento7 páginasPomr 1Afifa Prima GittaAinda não há avaliações
- Managing corticosteroids and their side effectsDocumento6 páginasManaging corticosteroids and their side effectsKrista Madranca CastroAinda não há avaliações
- Control of Nosocomial Infections by Data MiningDocumento4 páginasControl of Nosocomial Infections by Data MiningTI Journals PublishingAinda não há avaliações
- Ipcguide PDFDocumento194 páginasIpcguide PDFRoos WidiawatidewiAinda não há avaliações
- Salivary Gland DisordersDocumento50 páginasSalivary Gland DisordersghazyAinda não há avaliações
- A Day in The Life of A Clinical Research AssociateDocumento3 páginasA Day in The Life of A Clinical Research AssociateManjiri JoshiAinda não há avaliações
- CoolCut™ Series Shaver Blades and BurrsDocumento4 páginasCoolCut™ Series Shaver Blades and BurrsdcgAinda não há avaliações
- Comparison of Icd 10 and DSM 5: BY Anitha J I Mphil Clinical PsychologyDocumento102 páginasComparison of Icd 10 and DSM 5: BY Anitha J I Mphil Clinical Psychologyanitha1118Ainda não há avaliações
- Department of SurgeryDocumento8 páginasDepartment of SurgeryDeusah EzrahAinda não há avaliações
- Acyclovir antiviral drug overviewDocumento3 páginasAcyclovir antiviral drug overviewLisaAinda não há avaliações
- SV300 Service Training-Basic V1.0Documento82 páginasSV300 Service Training-Basic V1.0WALTER HUGO GOMEZAinda não há avaliações
- Spina Bifida OCCULTADocumento1 páginaSpina Bifida OCCULTArebelswanteddot_comAinda não há avaliações
- Protooncogene Tyrosineprotein Kinase Srcrelated Mouth Pyogenic Granuloma An Investigation Involving 2 InstanceskermbDocumento2 páginasProtooncogene Tyrosineprotein Kinase Srcrelated Mouth Pyogenic Granuloma An Investigation Involving 2 Instanceskermbsaucebelief33Ainda não há avaliações
- Suppurative Lung DIseaseDocumento33 páginasSuppurative Lung DIseaseNur Liyana Ahmad ZakiAinda não há avaliações
- Nonsteroidal Anti-Inflammatory Drugs (Nsaids) : Inhibition)Documento26 páginasNonsteroidal Anti-Inflammatory Drugs (Nsaids) : Inhibition)jemms16Ainda não há avaliações
- Health History and AssessmentDocumento2 páginasHealth History and AssessmentRalph Justin Tongos100% (1)
- Homoeopathic Perspective of Thyroid DisordersDocumento20 páginasHomoeopathic Perspective of Thyroid DisordersSaurav AroraAinda não há avaliações
- Treating Tetanus with InterventionDocumento2 páginasTreating Tetanus with InterventionChristopher John Aguelo100% (3)
- Elekta Infinity™ BrochureDocumento12 páginasElekta Infinity™ BrochureDC ShekharAinda não há avaliações
- Apollo Nashik PlansDocumento11 páginasApollo Nashik Plansjyoshnarath95% (21)
- Postpartum BluesDocumento17 páginasPostpartum BluesVeliani Putri anggrainiAinda não há avaliações