Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Principles of The Doctrine of ChristDocumento17 páginasPrinciples of The Doctrine of ChristNovus Blackstar100% (2)
- Models of Collaboration Between Education and ServicesDocumento17 páginasModels of Collaboration Between Education and ServicesSimran Josan100% (3)
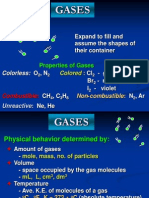
- Properties and Behavior of GasesDocumento34 páginasProperties and Behavior of GasesPaul Jeremiah Serrano NarvaezAinda não há avaliações
- Industrial Training (Tarun Kumar) - Final ReprtDocumento46 páginasIndustrial Training (Tarun Kumar) - Final ReprtSaumya GargAinda não há avaliações
- Guidelines For The Adminstration of Drugs Via Enteral Feeding TubesDocumento13 páginasGuidelines For The Adminstration of Drugs Via Enteral Feeding TubesDamodara Kumaran100% (3)
- Lesson Plan For DemoDocumento7 páginasLesson Plan For DemoShiela Tecson GamayonAinda não há avaliações
- Ewings Sarcoma - DescriptionDocumento3 páginasEwings Sarcoma - DescriptionDamodara KumaranAinda não há avaliações
- Jkms 20 687 PDFDocumento4 páginasJkms 20 687 PDFDamodara KumaranAinda não há avaliações
- Jkms 20 687 PDFDocumento4 páginasJkms 20 687 PDFDamodara KumaranAinda não há avaliações
- Breast ScreeningDocumento75 páginasBreast ScreeningDamodara KumaranAinda não há avaliações
- Recurrence Pattern - Oral CavityDocumento10 páginasRecurrence Pattern - Oral CavityDamodara KumaranAinda não há avaliações
- Medical Oncology SAQ Exam GuideDocumento7 páginasMedical Oncology SAQ Exam GuideguruyasAinda não há avaliações
- Interventions For The Treatment of Metastatic Extradural Spinal Cord Compression in Adults (Review)Documento48 páginasInterventions For The Treatment of Metastatic Extradural Spinal Cord Compression in Adults (Review)Damodara KumaranAinda não há avaliações
- Cranial Field CsiDocumento7 páginasCranial Field CsiDamodara KumaranAinda não há avaliações
- Current Issues in ResearchDocumento16 páginasCurrent Issues in ResearchDWolf67Ainda não há avaliações
- Radiation Therapy For Small-Cell Lung CancerDocumento13 páginasRadiation Therapy For Small-Cell Lung CancerDamodara KumaranAinda não há avaliações
- Cranial Field CsiDocumento7 páginasCranial Field CsiDamodara KumaranAinda não há avaliações
- Tumor Lysis SyndromeDocumento12 páginasTumor Lysis Syndromesanjuy gzzAinda não há avaliações
- Chemotherapy DrugsDocumento158 páginasChemotherapy DrugsDamodara KumaranAinda não há avaliações
- Whole Breast RT and APBIDocumento136 páginasWhole Breast RT and APBIDamodara KumaranAinda não há avaliações
- Occupational Therapy Post-Mastectomy English Mar 09r2Documento5 páginasOccupational Therapy Post-Mastectomy English Mar 09r2Damodara KumaranAinda não há avaliações
- LDR VR HDRDocumento8 páginasLDR VR HDRDamodara KumaranAinda não há avaliações
- Clin Management Tumor Lysis Web AlgorithmDocumento6 páginasClin Management Tumor Lysis Web AlgorithmDamodara KumaranAinda não há avaliações
- Surv PancreasDocumento8 páginasSurv PancreasDamodara KumaranAinda não há avaliações
- 5fu Vs Gem - JAMADocumento8 páginas5fu Vs Gem - JAMADamodara KumaranAinda não há avaliações
- Rectum ContouringDocumento14 páginasRectum ContouringDamodara KumaranAinda não há avaliações
- 5fu Vs Gem - JAMADocumento8 páginas5fu Vs Gem - JAMADamodara KumaranAinda não há avaliações
- Chapter #11: Volume #1Documento35 páginasChapter #11: Volume #1Mohamed MohamedAinda não há avaliações
- SPXDocumento6 páginasSPXapi-3700460Ainda não há avaliações
- Thesis NewDocumento55 páginasThesis NewHasan juwelAinda não há avaliações
- Emg 1204 Introduction To Materials Science Tutorial I Attempt All These Questions Question OneDocumento2 páginasEmg 1204 Introduction To Materials Science Tutorial I Attempt All These Questions Question Onesteve gateriAinda não há avaliações
- Tectonics, Vol. 8, NO. 5, PAGES 1015-1036, October 1989Documento22 páginasTectonics, Vol. 8, NO. 5, PAGES 1015-1036, October 1989atoinsepeAinda não há avaliações
- Plumbing Layout and SpecificationsDocumento1 páginaPlumbing Layout and SpecificationsLiza P. PaculanangAinda não há avaliações
- Cronbach AlphaDocumento15 páginasCronbach AlphaRendy EdistiAinda não há avaliações
- Lab No.7: Measurement of Coupling Coefficient, Directivity and Insertion Loss of A Directional CouplerDocumento3 páginasLab No.7: Measurement of Coupling Coefficient, Directivity and Insertion Loss of A Directional CouplerM. Ahmad RazaAinda não há avaliações
- Analyzing Visual TextsDocumento4 páginasAnalyzing Visual Textsapi-582845240Ainda não há avaliações
- ABV Testing Performa For ICF CoachesDocumento2 páginasABV Testing Performa For ICF Coachesmicell dieselAinda não há avaliações
- M and S - Capstone Marketing Across Cultures Fons TrompenaarsDocumento398 páginasM and S - Capstone Marketing Across Cultures Fons TrompenaarsBof BeosAinda não há avaliações
- Renold Transmission Chain Catalogue ENG 0112Documento94 páginasRenold Transmission Chain Catalogue ENG 0112nataliaAinda não há avaliações
- Should A Christian Believer Wear An ANKH?: Luxury Art By: Ketu'Rah GloreDocumento4 páginasShould A Christian Believer Wear An ANKH?: Luxury Art By: Ketu'Rah GloreMyk Twentytwenty NBeyondAinda não há avaliações
- Dada and Buddhist Thought - Sung-Won Ko PDFDocumento24 páginasDada and Buddhist Thought - Sung-Won Ko PDFJuan Manuel Gomez GarcíaAinda não há avaliações
- Ozone Layer EssayDocumento7 páginasOzone Layer Essayb71bpjha100% (2)
- Accenture Security RansomwareDocumento8 páginasAccenture Security RansomwareAbubakar Saddiq MusaAinda não há avaliações
- National Artists of the PhilippinesDocumento66 páginasNational Artists of the Philippinesshey mahilumAinda não há avaliações
- Nestle CompanyDocumento5 páginasNestle CompanymehakAinda não há avaliações
- Sample Management Representation Letter Type II SAS 70 AuditDocumento2 páginasSample Management Representation Letter Type II SAS 70 Auditaaldawi0% (1)
- Climate Change ReactionDocumento2 páginasClimate Change ReactionAngelika CotejoAinda não há avaliações
- Cable Drag ChainDocumento44 páginasCable Drag ChainsunhuynhAinda não há avaliações
- Visvesvaraya Technological University BelagaviDocumento148 páginasVisvesvaraya Technological University BelagavichetanbvAinda não há avaliações
- SAP Untangled: An Introductory Guide To SAP For New HomesDocumento28 páginasSAP Untangled: An Introductory Guide To SAP For New HomestempuserAinda não há avaliações
- Lab ReportDocumento11 páginasLab Reportkelvinkiplaa845Ainda não há avaliações
- The Photoconductive CellDocumento4 páginasThe Photoconductive Cellfasdasd123Ainda não há avaliações