Você também pode gostar
- Accessory TragusDocumento3 páginasAccessory TragusDeba P SarmaAinda não há avaliações
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocumento6 páginasAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaAinda não há avaliações
- Pilar Cyst With CrystalsDocumento2 páginasPilar Cyst With CrystalsDeba P SarmaAinda não há avaliações
- Acantholytic Bullous DiseaseDocumento4 páginasAcantholytic Bullous DiseaseDeba P SarmaAinda não há avaliações
- Acantholytic Dermatosis With DyskeratosisDocumento11 páginasAcantholytic Dermatosis With DyskeratosisDeba P SarmaAinda não há avaliações
- Acantholytic Acanthoma. M 60, ScrotumDocumento8 páginasAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaAinda não há avaliações
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Documento3 páginasAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaAinda não há avaliações
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Documento6 páginasBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaAinda não há avaliações
- Results of Search in Google Scholar On 'Deba P Sarma'Documento28 páginasResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaAinda não há avaliações
- Acantholytic Actinic KeratosisDocumento4 páginasAcantholytic Actinic KeratosisDeba P SarmaAinda não há avaliações
- Xanthogranuloma, M 30, Right ElbowDocumento4 páginasXanthogranuloma, M 30, Right ElbowDeba P SarmaAinda não há avaliações
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocumento7 páginasXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaAinda não há avaliações
- Verruca Vulgaris., M 22.,PPTDocumento2 páginasVerruca Vulgaris., M 22.,PPTDeba P SarmaAinda não há avaliações
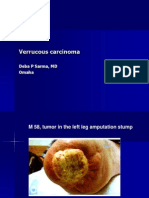
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocumento7 páginasVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaAinda não há avaliações
- Xanthogranuloma PPT DSDocumento9 páginasXanthogranuloma PPT DSDeba P SarmaAinda não há avaliações
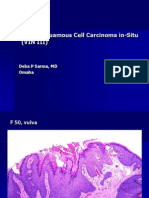
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocumento6 páginasVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaAinda não há avaliações
- Verrucous Epidermal Nevus. F 43, ScalpDocumento4 páginasVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaAinda não há avaliações
- Verrucous Carcinoma of The Foot, M 63, Left FootDocumento8 páginasVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Anatomy and Physiology of The SkinDocumento40 páginasAnatomy and Physiology of The SkinRicko Ciady100% (1)
- Freed TestimonyDocumento12 páginasFreed TestimonyCasey SeilerAinda não há avaliações
- Disaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Documento23 páginasDisaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Clara EverlastAinda não há avaliações
- Ravi Kota - DVLDocumento5 páginasRavi Kota - DVLAbhishek Sinha RoyAinda não há avaliações
- Ebook Spine Secrets PDF Full Chapter PDFDocumento67 páginasEbook Spine Secrets PDF Full Chapter PDFgregory.cross110100% (23)
- HEM-FO-01&02, Rev.02 - ID FormsDocumento1 páginaHEM-FO-01&02, Rev.02 - ID FormsHazelle karren ManabatAinda não há avaliações
- Dr.G.Thiruvenkadam Post Graduate Department of Pediatric & Preventive DentistryDocumento55 páginasDr.G.Thiruvenkadam Post Graduate Department of Pediatric & Preventive Dentistryதிருவேங்கடம் கோபாலன்Ainda não há avaliações
- Winning Piece FeatureDocumento9 páginasWinning Piece FeatureHowardAinda não há avaliações
- Employees' State Insurance Corporation: Esic Hospital, Udyogamandal Udyogamandal P.O., Ernakulam, Kerala-683 501Documento4 páginasEmployees' State Insurance Corporation: Esic Hospital, Udyogamandal Udyogamandal P.O., Ernakulam, Kerala-683 501Kirankumar MutnaliAinda não há avaliações
- STSurg NumntDocumento11 páginasSTSurg NumntrohiAinda não há avaliações
- CBT Ortho 1Documento45 páginasCBT Ortho 1putri umepalAinda não há avaliações
- Anal FissureDocumento1 páginaAnal Fissureshailesh284Ainda não há avaliações
- StatusDocumento3 páginasStatusjobertAinda não há avaliações
- Managing Otitis ExternaDocumento6 páginasManaging Otitis ExternaChitaAinda não há avaliações
- Fixation of Mandibular Fractures With 2.0 MM MiniplatesDocumento7 páginasFixation of Mandibular Fractures With 2.0 MM MiniplatesRajan KarmakarAinda não há avaliações
- National Board Dental ExaminationDocumento2 páginasNational Board Dental Examinationjyoti rawatAinda não há avaliações
- Exotic Animal Medicine For The Veterinary Technician PDFDocumento2 páginasExotic Animal Medicine For The Veterinary Technician PDFJoshuaAinda não há avaliações
- 4 Stages of AnesthesiaDocumento1 página4 Stages of Anesthesialfa6435514Ainda não há avaliações
- Ankle ExerciseDocumento2 páginasAnkle Exercisepocholofiesta20048772Ainda não há avaliações
- Cardiac Action PotentialDocumento5 páginasCardiac Action PotentialjayAinda não há avaliações
- AcneDocumento38 páginasAcneSavanna ChambersAinda não há avaliações
- Completing The Partogram in Pregnancy 5.0Documento9 páginasCompleting The Partogram in Pregnancy 5.0fei cuaAinda não há avaliações
- Pulpotomy VitalDocumento5 páginasPulpotomy VitalRachael VincentAinda não há avaliações
- World Health OrganizationDocumento2 páginasWorld Health OrganizationMarathi CalligraphyAinda não há avaliações
- Basic Neuroanatomy PPT SlidesDocumento21 páginasBasic Neuroanatomy PPT SlidesSuphadetch Leung100% (1)
- Personal Care-Cleansing and Dressing, Skin Care Case History-Mrs. Mcbride New Vocabulary and Difficult WordsDocumento4 páginasPersonal Care-Cleansing and Dressing, Skin Care Case History-Mrs. Mcbride New Vocabulary and Difficult Wordsnadya wahyuAinda não há avaliações
- Information Sheet For Applicants For Employers of Indonesia Candidates For "Kangoshi"Documento11 páginasInformation Sheet For Applicants For Employers of Indonesia Candidates For "Kangoshi"bnp2tkidotgodotidAinda não há avaliações
- 3 3 2 A Med History 3 2Documento2 páginas3 3 2 A Med History 3 2api-263196423Ainda não há avaliações
- Essential Anesthesia From Science To Practice,.46Documento1 páginaEssential Anesthesia From Science To Practice,.46Jean PaulAinda não há avaliações
- Direction: Kurnihayati, M.PDDocumento28 páginasDirection: Kurnihayati, M.PDKurnihayati MuklasAinda não há avaliações