Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Post Concussion SyndromeDocumento2 páginasPost Concussion SyndromeCeleborn021100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Essential Sports MedicineDocumento466 páginasEssential Sports MedicineMaria Alejandra HurtadoAinda não há avaliações
- Concussion Guideline 3rd Edition FinalDocumento250 páginasConcussion Guideline 3rd Edition FinalGus LionsAinda não há avaliações
- Head InjuryDocumento7 páginasHead InjuryRoshan Ghimire100% (1)
- Oet 2.0 Practice Tests ListeningDocumento60 páginasOet 2.0 Practice Tests ListeningLorraine Johns0% (1)
- 2020 MedicalCertificate (Combative)Documento1 página2020 MedicalCertificate (Combative)Dennmark IgutAinda não há avaliações
- Marshall 2015Documento13 páginasMarshall 2015MalikinNadalAinda não há avaliações
- PE11 Q4 Module4a Weeks1and2Documento20 páginasPE11 Q4 Module4a Weeks1and2Kristelle BigawAinda não há avaliações
- English For Specific Purposes VeterinarianDocumento25 páginasEnglish For Specific Purposes VeterinarianChristopher Mccandless83% (6)
- MCPS Sports Concussion Data 2014-15Documento1 páginaMCPS Sports Concussion Data 2014-15Concussion_MCPS_MdAinda não há avaliações
- Brain Sentry Inova Football Helmet Sensor Research Study ProposalDocumento5 páginasBrain Sentry Inova Football Helmet Sensor Research Study ProposalConcussion_MCPS_MdAinda não há avaliações
- Parent Letter To MCPS Re Student Injury Data - 01-14-2015Documento11 páginasParent Letter To MCPS Re Student Injury Data - 01-14-2015Concussion_MCPS_MdAinda não há avaliações
- NFL 2010 Letter Re Concussion LegDocumento2 páginasNFL 2010 Letter Re Concussion LegConcussion_MCPS_MdAinda não há avaliações
- MCPS (MD) Tobacco-Free SCH PolicyDocumento2 páginasMCPS (MD) Tobacco-Free SCH PolicyConcussion_MCPS_MdAinda não há avaliações
- MCPS Student Injury Report FormDocumento2 páginasMCPS Student Injury Report FormConcussion_MCPS_MdAinda não há avaliações
- Template 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Documento1 páginaTemplate 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Concussion_MCPS_MdAinda não há avaliações
- MD Bill - HS Football Helmet Sensor Pilot ProgramDocumento6 páginasMD Bill - HS Football Helmet Sensor Pilot ProgramConcussion_MCPS_MdAinda não há avaliações
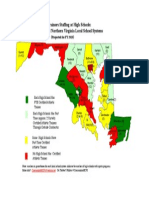
- Projected Ath Trainer HS Staffing in FY 2015-Map of MD and N. VA CountiesDocumento1 páginaProjected Ath Trainer HS Staffing in FY 2015-Map of MD and N. VA CountiesConcussion_MCPS_MdAinda não há avaliações
- Piaa FormDocumento9 páginasPiaa Formapi-325520279Ainda não há avaliações
- Coach Exam Questions-KumiteDocumento6 páginasCoach Exam Questions-Kumitemalicia3Ainda não há avaliações
- Sports-Related Concussions: What Can Happen in The Long Run?Documento10 páginasSports-Related Concussions: What Can Happen in The Long Run?Hannah ReedAinda não há avaliações
- Head Injury Management of PediatricDocumento22 páginasHead Injury Management of PediatricIrma KusumaAinda não há avaliações
- Concussions PowerpointDocumento15 páginasConcussions Powerpointapi-240817936Ainda não há avaliações
- Concussion Management PlanDocumento4 páginasConcussion Management Planapi-310029510Ainda não há avaliações
- Child SCAT5Documento8 páginasChild SCAT5KinesiuzAinda não há avaliações
- The Morning Calm Korea Weekly - Sep. 7, 2007Documento24 páginasThe Morning Calm Korea Weekly - Sep. 7, 2007Morning Calm Weekly Newspaper100% (5)
- Jesse Goedman The Proposal 16 14Documento3 páginasJesse Goedman The Proposal 16 14api-381484612Ainda não há avaliações
- Sports Injury ManagementDocumento8 páginasSports Injury Management8m9vv5b6h7Ainda não há avaliações
- Tyler Procious - Research Study AnalysisDocumento2 páginasTyler Procious - Research Study Analysisapi-537717726Ainda não há avaliações
- Argumentative Essay FinalDocumento3 páginasArgumentative Essay Finalapi-248602269Ainda não há avaliações
- CSE 598 U2 Sport Concussion Assessment System Project Overview DocumentDocumento6 páginasCSE 598 U2 Sport Concussion Assessment System Project Overview DocumentjamesbeebeAinda não há avaliações
- Eduskills Listening Mock Test Day 3 QNDocumento15 páginasEduskills Listening Mock Test Day 3 QNselvarajmarithai1432Ainda não há avaliações
- Isai Arasi News Journal ArticleDocumento8 páginasIsai Arasi News Journal ArticlenamdevnnayakAinda não há avaliações
- 04 Huang v. Philippine Hoteliers, Inc, G.R. No. 180440, 5 December 2012Documento15 páginas04 Huang v. Philippine Hoteliers, Inc, G.R. No. 180440, 5 December 2012Andrei Da JoseAinda não há avaliações
- Efa 2009 UploadDocumento87 páginasEfa 2009 Uploadrobjones21Ainda não há avaliações
- 2015 - Two Baselines Are Better Than One - Improving The Reliability of Computerized Testing in Sports NeuropsychologyDocumento8 páginas2015 - Two Baselines Are Better Than One - Improving The Reliability of Computerized Testing in Sports NeuropsychologyRaúl VerdugoAinda não há avaliações
- Curs 2-Managementul Pacientului Cu TCCDocumento46 páginasCurs 2-Managementul Pacientului Cu TCCMarina ApostolAinda não há avaliações
- Concussion PPT June 20101Documento36 páginasConcussion PPT June 20101CiiFitriAinda não há avaliações
- 2013 Physical Form English UIL-AISDDocumento4 páginas2013 Physical Form English UIL-AISDDavid JimenezAinda não há avaliações