Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Performance Management Systems and Strategies by Dipak Kumar BhattacharyyaDocumento385 páginasPerformance Management Systems and Strategies by Dipak Kumar Bhattacharyyasayal96amrit100% (3)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Unit 5-People Should Manage Nature-Ts-Planning Guide-Grade 5Documento1 páginaUnit 5-People Should Manage Nature-Ts-Planning Guide-Grade 5api-457240136Ainda não há avaliações
- Attention: 6R60/6R75/6R80 Installation GuideDocumento4 páginasAttention: 6R60/6R75/6R80 Installation GuideEdwinferAinda não há avaliações
- ASWP Manual - Section 1 - IntroductionDocumento17 páginasASWP Manual - Section 1 - Introductionjmvm56Ainda não há avaliações
- Ssg-Ng01012401-Gen-Aa-5880-00012 - C01 - Ssags Nigerian Content PlanDocumento24 páginasSsg-Ng01012401-Gen-Aa-5880-00012 - C01 - Ssags Nigerian Content PlanStroom Limited100% (2)
- Science 10 FINAL Review 2014Documento49 páginasScience 10 FINAL Review 2014Zara Zalaal [Student]Ainda não há avaliações
- Chapter 04 - Motion and Force - DynamicsDocumento24 páginasChapter 04 - Motion and Force - DynamicsMohamad SyazwanAinda não há avaliações
- Writing Capstone Research Project For Senior High School A Modified Guide ManualDocumento9 páginasWriting Capstone Research Project For Senior High School A Modified Guide ManualIOER International Multidisciplinary Research Journal ( IIMRJ)Ainda não há avaliações
- International Standard: Iso/Iec 7816-2Documento16 páginasInternational Standard: Iso/Iec 7816-2Anwar MohamedAinda não há avaliações
- SalivaDocumento42 páginasSalivaAtharva KambleAinda não há avaliações
- Vững vàng nền tảng, Khai sáng tương lai: Trang - 1Documento11 páginasVững vàng nền tảng, Khai sáng tương lai: Trang - 1An AnAinda não há avaliações
- Unit-4.Vector CalculusDocumento32 páginasUnit-4.Vector Calculuskhatua.deb87Ainda não há avaliações
- Fulltext PDFDocumento454 páginasFulltext PDFVirmantas JuoceviciusAinda não há avaliações
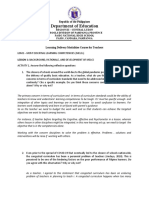
- Department of Education: Republic of The PhilippinesDocumento6 páginasDepartment of Education: Republic of The PhilippinesLalaine QuitoAinda não há avaliações
- Dede - (2010) - Comparing Frameworks For 21st Century Skills PDFDocumento16 páginasDede - (2010) - Comparing Frameworks For 21st Century Skills PDFNaing Lynn HtunAinda não há avaliações
- Mindset For IELTS Level 1 Student's Book PDF English As A Second or Foreign Language International English Language TestinDocumento1 páginaMindset For IELTS Level 1 Student's Book PDF English As A Second or Foreign Language International English Language TestinhiAinda não há avaliações
- Jesoc5 1 PDFDocumento15 páginasJesoc5 1 PDFfaisal3096Ainda não há avaliações
- 007: The Stealth Affair ManualDocumento11 páginas007: The Stealth Affair Manualcodigay769Ainda não há avaliações
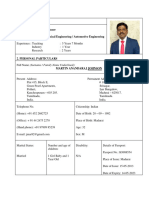
- CV (Martin A Johnson)Documento7 páginasCV (Martin A Johnson)kganesanAinda não há avaliações
- Authority To TravelDocumento39 páginasAuthority To TraveljoraldAinda não há avaliações
- EASA CS-22 Certification of SailplanesDocumento120 páginasEASA CS-22 Certification of SailplanessnorrigAinda não há avaliações
- American J Political Sci - 2023 - Eggers - Placebo Tests For Causal InferenceDocumento16 páginasAmerican J Political Sci - 2023 - Eggers - Placebo Tests For Causal Inferencemarta bernardiAinda não há avaliações
- Unit-I Basic Concepts: Course Code: BTCS9504 Course Name: Network Operating SystemsDocumento17 páginasUnit-I Basic Concepts: Course Code: BTCS9504 Course Name: Network Operating SystemsPradeep BediAinda não há avaliações
- Brochure Mastertile TilingDocumento48 páginasBrochure Mastertile TilingMaha Mufleh100% (1)
- Landis+Gyr Model EM5300 Class 0.5 Electricity Meter 14-2-63Documento5 páginasLandis+Gyr Model EM5300 Class 0.5 Electricity Meter 14-2-63kulukundunguAinda não há avaliações
- V3 Tool Installation GuideDocumento13 páginasV3 Tool Installation GuideLeonardo Floresta NascimentoAinda não há avaliações
- WCDMA19 Prfile Descriptions W19P8 08A APPRDocumento254 páginasWCDMA19 Prfile Descriptions W19P8 08A APPRoaguilar83Ainda não há avaliações
- Bike LanesDocumento12 páginasBike LanesChitikala RajeshAinda não há avaliações
- Australia Visa RequirementsDocumento1 páginaAustralia Visa RequirementsJoana DetomasAinda não há avaliações
- CH 11 International TradeDocumento20 páginasCH 11 International TradeSANTU GHORAIAinda não há avaliações