Você também pode gostar
- Abortion and Sterilization: Medical and Social AspectsNo EverandAbortion and Sterilization: Medical and Social AspectsJane E. HodgsonAinda não há avaliações
- Non Obstetric Surgery During Pregnancy 2013Documento51 páginasNon Obstetric Surgery During Pregnancy 2013christietwongAinda não há avaliações
- Complicated Labor and DeliveryDocumento226 páginasComplicated Labor and Deliveryrhimineecat71100% (1)
- B Lynch SuturingDocumento32 páginasB Lynch SuturingDoru Draghici67% (3)
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocumento39 páginasObstetric Anal Sphincter Injury (OASIS) - UpToDateErickAinda não há avaliações
- Claire Maevelle A. Laxamana BSP - 3ADocumento10 páginasClaire Maevelle A. Laxamana BSP - 3ACLaire Maevelle Angeles LaxamanaAinda não há avaliações
- Cardiac Disease in PregnancyDocumento28 páginasCardiac Disease in PregnancyviharadewiAinda não há avaliações
- Singer and Monaghan's Cervical and Lower Genital Tract Precancer: Diagnosis and TreatmentNo EverandSinger and Monaghan's Cervical and Lower Genital Tract Precancer: Diagnosis and TreatmentNota: 5 de 5 estrelas5/5 (1)
- Handbook of Current and Novel Protocols for the Treatment of InfertilityNo EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanAinda não há avaliações
- Heparin Induced ThrombocytopeniaDocumento17 páginasHeparin Induced ThrombocytopeniaTafsir arefin100% (1)
- A System of Operative Surgery, Volume IV (of 4)No EverandA System of Operative Surgery, Volume IV (of 4)Nota: 4 de 5 estrelas4/5 (1)
- Urinary System: Cytology, Histology, Cystoscopy, and RadiologyNo EverandUrinary System: Cytology, Histology, Cystoscopy, and RadiologyAinda não há avaliações
- Bladder IrrigationDocumento9 páginasBladder IrrigationWelas_Riyanto_9968Ainda não há avaliações
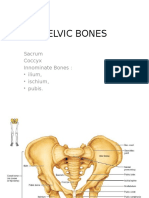
- Pelvic BoneDocumento15 páginasPelvic BoneYoanneveline TanakAinda não há avaliações
- Cardiac Disease in PregnancyDocumento21 páginasCardiac Disease in PregnancyRenata CilestrinaAinda não há avaliações
- Scrotoscopic SurgeryNo EverandScrotoscopic SurgeryJinrui YangAinda não há avaliações
- 2023 OB/GYN Coding Manual: Components of Correct CodingNo Everand2023 OB/GYN Coding Manual: Components of Correct CodingAinda não há avaliações
- Fetal Physiological Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological MeasurementsNo EverandFetal Physiological Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological MeasurementsPeter RolfeAinda não há avaliações
- PA Genitalia WanitaDocumento100 páginasPA Genitalia WanitaBAinda não há avaliações
- Radiology and Follow-up of Urologic SurgeryNo EverandRadiology and Follow-up of Urologic SurgeryAinda não há avaliações
- Perinatal Medicine: Clinical and Biochemical Aspects of the Evaluation, Diagnosis and Management of the Fetus and NewbornNo EverandPerinatal Medicine: Clinical and Biochemical Aspects of the Evaluation, Diagnosis and Management of the Fetus and NewbornAinda não há avaliações
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Benign and Malignant Tumors of Female Genital TractDocumento14 páginasBenign and Malignant Tumors of Female Genital TractDimitrios PapadopoulosAinda não há avaliações
- Ectopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentDocumento43 páginasEctopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentAlrick AsentistaAinda não há avaliações
- MK Fetal Lie and Presentation (OBGY)Documento9 páginasMK Fetal Lie and Presentation (OBGY)Moses Jr KazevuAinda não há avaliações
- Benign Disease of The UterusDocumento27 páginasBenign Disease of The UterusnyangaraAinda não há avaliações
- FCE OB GYN 2007 Male 2nd RoatationDocumento8 páginasFCE OB GYN 2007 Male 2nd Roatationapi-3763146Ainda não há avaliações
- HysterosDocumento17 páginasHysterosAnto PopaAinda não há avaliações
- Ambulatory HysterosDocumento8 páginasAmbulatory Hysteroskomlanihou_890233161100% (1)
- The Chinese University of Hong Kong Obstetrics and Gynaecology Module Student Handbook 2016-2017Documento37 páginasThe Chinese University of Hong Kong Obstetrics and Gynaecology Module Student Handbook 2016-2017Ken100% (1)
- GCT For Dummies - Publish AbleDocumento24 páginasGCT For Dummies - Publish AblepcrosleyAinda não há avaliações
- C SectionDocumento50 páginasC SectionAlano S. LimgasAinda não há avaliações
- Dopplerinpregnancy 130823082426 Phpapp02Documento64 páginasDopplerinpregnancy 130823082426 Phpapp02Herry SasukeAinda não há avaliações
- Female Reproductive SystemDocumento8 páginasFemale Reproductive SystemEfanPutraAinda não há avaliações
- Lecture 6 Breach Presentation Transversal Oblique LieDocumento51 páginasLecture 6 Breach Presentation Transversal Oblique Lietanmai nooluAinda não há avaliações
- Uterine FibroidsDocumento21 páginasUterine FibroidsPrasun BiswasAinda não há avaliações
- Cervical Intraepithelial Neoplasia and Cervical CancerDocumento28 páginasCervical Intraepithelial Neoplasia and Cervical CancerNatnael100% (1)
- Acute Abdomen During Pregnancy BelaynehDocumento47 páginasAcute Abdomen During Pregnancy BelaynehYohannis AsefaAinda não há avaliações
- Tog Journal 2016Documento61 páginasTog Journal 2016thevijay007100% (1)
- Basic Thyroid ExaminationDocumento6 páginasBasic Thyroid ExaminationPalwasha MalikAinda não há avaliações
- Nancy E Fay MD Facog Division of Reproductive MedicineDocumento32 páginasNancy E Fay MD Facog Division of Reproductive MedicineAdityo MulyonoAinda não há avaliações
- (Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDocumento10 páginas(Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDexter IanAinda não há avaliações
- Omphalocele & Gastroschisis - SNguyenDocumento21 páginasOmphalocele & Gastroschisis - SNguyenherdigunantaAinda não há avaliações
- Benign Lesions of Vulva and VaginaDocumento34 páginasBenign Lesions of Vulva and VaginaCabdiAinda não há avaliações
- Miscarriage Early Pregnancy LossDocumento10 páginasMiscarriage Early Pregnancy LossiwennieAinda não há avaliações
- Thrombocytopenia in PregnancyDocumento31 páginasThrombocytopenia in Pregnancyari naAinda não há avaliações
- GTG 37bDocumento32 páginasGTG 37bKadelsy BristolAinda não há avaliações
- Cervical CancerDocumento30 páginasCervical Cancerhuhknee100% (1)
- E. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborDocumento10 páginasE. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborSK ASIF ALIAinda não há avaliações
- Obstetrics and Gynecological InstrumentsDocumento31 páginasObstetrics and Gynecological InstrumentsGAYATHRI RAKESHAinda não há avaliações
- RCOG Cardiac Disease and Pregnancy PDFDocumento18 páginasRCOG Cardiac Disease and Pregnancy PDFSteven SetioAinda não há avaliações
- Cervical CancerDocumento50 páginasCervical CancerMohmmadRjab SederAinda não há avaliações
- Abortion KuliahDocumento38 páginasAbortion KuliahElsa Hasibuan100% (1)
- WHO PPHDocumento62 páginasWHO PPHAchyut SharmaAinda não há avaliações
- Spontaneous Vaginal Delivery IN Post Term PregnancyDocumento55 páginasSpontaneous Vaginal Delivery IN Post Term Pregnancyr.pavinvikneshAinda não há avaliações
- Fetal Growth Restriction - ACOG 2019Documento23 páginasFetal Growth Restriction - ACOG 2019Adhitya Yudha MaulanaAinda não há avaliações
- TechBridge TCP ServiceNow Business Case - Group 6Documento9 páginasTechBridge TCP ServiceNow Business Case - Group 6Takiyah Shealy100% (1)
- Driver Drowsiness Detection System Using Raspberry PiDocumento7 páginasDriver Drowsiness Detection System Using Raspberry PiIJRASETPublicationsAinda não há avaliações
- Fortnite Task Courier Pack 1500 V Bucks - BuscarDocumento1 páginaFortnite Task Courier Pack 1500 V Bucks - Buscariancard321Ainda não há avaliações
- Peanut AllergyDocumento4 páginasPeanut AllergyLNICCOLAIOAinda não há avaliações
- Index: © Christopher Pitt 2018 C. Pitt, The Definitive Guide To AdonisjsDocumento5 páginasIndex: © Christopher Pitt 2018 C. Pitt, The Definitive Guide To AdonisjsZidi BoyAinda não há avaliações
- This Is A Short Presentation To Explain The Character of Uncle Sam, Made by Ivo BogoevskiDocumento7 páginasThis Is A Short Presentation To Explain The Character of Uncle Sam, Made by Ivo BogoevskiIvo BogoevskiAinda não há avaliações
- MegaMacho Drums BT READ MEDocumento14 páginasMegaMacho Drums BT READ MEMirkoSashaGoggoAinda não há avaliações
- Fce Use of English 1 Teacher S Book PDFDocumento2 páginasFce Use of English 1 Teacher S Book PDFOrestis GkaloAinda não há avaliações
- Rdramirez Aota 2018 Poster For PortfolioDocumento1 páginaRdramirez Aota 2018 Poster For Portfolioapi-437843157Ainda não há avaliações
- 4039-Texto Del Artículo-12948-3-10-20211123Documento14 páginas4039-Texto Del Artículo-12948-3-10-20211123Ricardo ApazaAinda não há avaliações
- SHS G11 Reading and Writing Q3 Week 1 2 V1Documento15 páginasSHS G11 Reading and Writing Q3 Week 1 2 V1Romeo Espinosa Carmona JrAinda não há avaliações
- Our Story Needs No Filter by Nagarkar SudeepDocumento153 páginasOur Story Needs No Filter by Nagarkar SudeepKavya SunderAinda não há avaliações
- Dependent ClauseDocumento28 páginasDependent ClauseAndi Febryan RamadhaniAinda não há avaliações
- SY22-23+Annual+Report FinalDocumento47 páginasSY22-23+Annual+Report FinalNorus LizaAinda não há avaliações
- Introduction Spreadable Media TtsDocumento22 páginasIntroduction Spreadable Media TtsYanro FerrerAinda não há avaliações
- Gobekli TepeDocumento2 páginasGobekli TepeCarl Feagans100% (1)
- Brain Injury Patients Have A Place To Be Themselves: WHY WHYDocumento24 páginasBrain Injury Patients Have A Place To Be Themselves: WHY WHYDonna S. SeayAinda não há avaliações
- Final SEC Judgment As To Defendant Michael Brauser 3.6.20Documento14 páginasFinal SEC Judgment As To Defendant Michael Brauser 3.6.20Teri BuhlAinda não há avaliações
- What Is The PCB Shelf Life Extending The Life of PCBsDocumento9 páginasWhat Is The PCB Shelf Life Extending The Life of PCBsjackAinda não há avaliações
- Sheetal PatilDocumento4 páginasSheetal PatilsheetalAinda não há avaliações
- Operating Instructions: Rotary Lobe PumpDocumento77 páginasOperating Instructions: Rotary Lobe PumpRuslan SlusarAinda não há avaliações
- Writ Petition 21992 of 2019 FinalDocumento22 páginasWrit Petition 21992 of 2019 FinalNANDANI kumariAinda não há avaliações
- Learning English Through The Educational Games of Wordwall Website For Elementary Students by Group 1 (R4E)Documento6 páginasLearning English Through The Educational Games of Wordwall Website For Elementary Students by Group 1 (R4E)NurulAinda não há avaliações
- Unit 1 Bearer PlantsDocumento2 páginasUnit 1 Bearer PlantsEmzAinda não há avaliações
- Case ColorscopeDocumento7 páginasCase ColorscopeRatin MathurAinda não há avaliações
- Overlay Control PlansDocumento1 páginaOverlay Control PlansSTS-SPARK GAMINGAinda não há avaliações
- 95-03097 Ballvlv300350 WCB PDFDocumento26 páginas95-03097 Ballvlv300350 WCB PDFasitdeyAinda não há avaliações
- Diesel Engines For Vehicles D2066 D2676Documento6 páginasDiesel Engines For Vehicles D2066 D2676Branislava Savic63% (16)
- Docket - CDB Batu GajahDocumento1 páginaDocket - CDB Batu Gajahfatin rabiatul adawiyahAinda não há avaliações
- Revenue Memorandum Circular No. 55-2016: For ExampleDocumento2 páginasRevenue Memorandum Circular No. 55-2016: For ExampleFedsAinda não há avaliações