Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Useful Vocabs For OET Writing & Speaking PDFDocumento2 páginasUseful Vocabs For OET Writing & Speaking PDFLiju K Oommen100% (3)
- Module 3 - Nursing Assessment in Family Nursing PracticeDocumento7 páginasModule 3 - Nursing Assessment in Family Nursing PracticeRogedith DelaRosaAinda não há avaliações
- Planning For A Health Career: Unit 4Documento34 páginasPlanning For A Health Career: Unit 4Lanie Tamacio BadayAinda não há avaliações
- Running Head: Evidence-Based Practice: Pressure Ulcer RiskDocumento5 páginasRunning Head: Evidence-Based Practice: Pressure Ulcer RiskElise HowardAinda não há avaliações
- Lesson Plan For COT First QuarterDocumento4 páginasLesson Plan For COT First QuarterJunnel Maravilla100% (1)
- Sanford Chris CVDocumento9 páginasSanford Chris CVChris SanfordAinda não há avaliações
- Medicine Lec.9 - Viral Infection IIDocumento42 páginasMedicine Lec.9 - Viral Infection II7fefdfbea1Ainda não há avaliações
- M. Sc. Nursing Programme Analysis: Post-Graduate Education-Msc NursingDocumento11 páginasM. Sc. Nursing Programme Analysis: Post-Graduate Education-Msc NursingMallika JoonAinda não há avaliações
- Steps in Viral Pathogenesis-Lecture ThreeDocumento3 páginasSteps in Viral Pathogenesis-Lecture ThreeIM CTAinda não há avaliações
- The Psychiatric Review of Symptoms - A Screening Tool For Family Physicians - American Family PhysicianDocumento7 páginasThe Psychiatric Review of Symptoms - A Screening Tool For Family Physicians - American Family PhysicianTimothy TurscakAinda não há avaliações
- Bells Palsy Handbook Facial Nerve Palsy or Bells Palsy Facial Paralysis Causes, Symptoms, Treatment, Face Exercises ... (Alan MC Donald DR Alexa Smith) (Z-Library)Documento94 páginasBells Palsy Handbook Facial Nerve Palsy or Bells Palsy Facial Paralysis Causes, Symptoms, Treatment, Face Exercises ... (Alan MC Donald DR Alexa Smith) (Z-Library)mayakhoAinda não há avaliações
- An Impression Technique For Patients With Fixed Orthodontic AppliancesDocumento2 páginasAn Impression Technique For Patients With Fixed Orthodontic Appliancesmoji_puiAinda não há avaliações
- Case Study: Epidemiology LaboratoryDocumento5 páginasCase Study: Epidemiology LaboratoryDonna IlarAinda não há avaliações
- Better Strategies For Covid VaccinationsDocumento8 páginasBetter Strategies For Covid VaccinationsMiguel Angel Vilar HerreroAinda não há avaliações
- Knowledge, Attitude and Practice of Cancer Screening Among Health Care Professionals in A Central Hospital in NepalDocumento8 páginasKnowledge, Attitude and Practice of Cancer Screening Among Health Care Professionals in A Central Hospital in NepalBruce LennyAinda não há avaliações
- Chapter 1 Lesson 1Documento8 páginasChapter 1 Lesson 1Aizel ManiagoAinda não há avaliações
- Robsons Ten Group Classification of Cesarean Section at A Tertiary Center in NepalDocumento6 páginasRobsons Ten Group Classification of Cesarean Section at A Tertiary Center in NepalgehanathAinda não há avaliações
- Manangan, Eugene B. - FDAR Boggy UterusDocumento2 páginasManangan, Eugene B. - FDAR Boggy UterusGin MananganAinda não há avaliações
- Observational Studies Lecture - ReviewDocumento3 páginasObservational Studies Lecture - ReviewKelsey AndersonAinda não há avaliações
- Caries TimelineDocumento11 páginasCaries TimelineManuelRomeroFAinda não há avaliações
- Guidelines For Toxicity/safety Profile Evaluation of Ayurved & Siddha, Plant DrugsDocumento5 páginasGuidelines For Toxicity/safety Profile Evaluation of Ayurved & Siddha, Plant DrugsPRAKASH DESHPANDEAinda não há avaliações
- Fellowship Accreditation in Pediatric Otolaryngology: A Review of The IssuesDocumento5 páginasFellowship Accreditation in Pediatric Otolaryngology: A Review of The IssuesDeepBhattacharyyaAinda não há avaliações
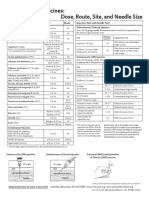
- Injection Site and Needle Size Vaccine Dose RouteDocumento1 páginaInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaAinda não há avaliações
- BG Group Standard Health Management BG-ST-HR-SER-004 (HSSE Management System Framework Section 9.1.3)Documento18 páginasBG Group Standard Health Management BG-ST-HR-SER-004 (HSSE Management System Framework Section 9.1.3)Sunday Augustine ChibuzoAinda não há avaliações
- Breast LumpDocumento4 páginasBreast LumpYoussef Refaat RaoofAinda não há avaliações
- Medical MycologyDocumento10 páginasMedical MycologyNive KojAinda não há avaliações
- Konsulta ItrDocumento1 páginaKonsulta ItrBarangay DanaoAinda não há avaliações
- Eform For Players Cluster MeetDocumento8 páginasEform For Players Cluster Meetseph bronAinda não há avaliações
- Pedia Tickler Update 2017Documento2 páginasPedia Tickler Update 2017Tani BokAinda não há avaliações
- What Is Brain CancerDocumento3 páginasWhat Is Brain Canceryash vardhanAinda não há avaliações