Você também pode gostar
- Oral Wound Healing: Cell Biology and Clinical ManagementNo EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaAinda não há avaliações
- Mucosa in Complete DenturesDocumento4 páginasMucosa in Complete Denturesspu123Ainda não há avaliações
- Regressive Changes of TeethDocumento45 páginasRegressive Changes of TeethNader AlaizariAinda não há avaliações
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocumento39 páginasAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyAinda não há avaliações
- RPD ImpressionDocumento49 páginasRPD ImpressionAmar Bimavarapu0% (1)
- 11 - Novel Decision Tree Algorithms For The Treatment Planning of Compromised TeethDocumento10 páginas11 - Novel Decision Tree Algorithms For The Treatment Planning of Compromised TeethkochikaghochiAinda não há avaliações
- Impression Materials For Partial DentureDocumento40 páginasImpression Materials For Partial Dentureyunie0959Ainda não há avaliações
- Pediatric Dental PatientDocumento125 páginasPediatric Dental PatientHebah NawafAinda não há avaliações
- Mandibular Central IncisorDocumento19 páginasMandibular Central IncisorDR. ISHITA SINGHAL100% (1)
- Treatment For ChildrenDocumento66 páginasTreatment For ChildrenMohsin HabibAinda não há avaliações
- Primary ImpressionDocumento18 páginasPrimary ImpressionJewana J. Ghazal67% (3)
- Space MaintainerDocumento13 páginasSpace MaintainerAnamAinda não há avaliações
- Dentin Bonding Agents - An OverviewDocumento4 páginasDentin Bonding Agents - An OverviewIOSRjournalAinda não há avaliações
- Concepts of Enamel and Dentin AdhesionDocumento12 páginasConcepts of Enamel and Dentin Adhesionizeldien5870Ainda não há avaliações
- Dental PostDocumento43 páginasDental PostKair Hope TweetAinda não há avaliações
- Digital Impressions - A Review of Latest PDFDocumento5 páginasDigital Impressions - A Review of Latest PDFSonali KinikarAinda não há avaliações
- Fundamentals of Tooth PreparationDocumento6 páginasFundamentals of Tooth PreparationAnamika PandeyAinda não há avaliações
- Surgical Endodontics 2012Documento11 páginasSurgical Endodontics 2012grzeniouAinda não há avaliações
- Badly Broken MarzoukDocumento68 páginasBadly Broken MarzoukHend MohamedAinda não há avaliações
- Lecture 2 Tooth Eruption and SheddingDocumento35 páginasLecture 2 Tooth Eruption and SheddingAMIT GUPTAAinda não há avaliações
- Regenerative Endodontics Part 2Documento118 páginasRegenerative Endodontics Part 2rasagna reddyAinda não há avaliações
- CHAPTER 13. Interdisciplinary ConsiderationsDocumento13 páginasCHAPTER 13. Interdisciplinary ConsiderationsAlina AnechiteiAinda não há avaliações
- Mccracken'S Removable Partial Prosthodontics. Chapter 10 & 19Documento50 páginasMccracken'S Removable Partial Prosthodontics. Chapter 10 & 19Al CarLozAinda não há avaliações
- Tarnish - CorrosionDocumento18 páginasTarnish - CorrosionAmniAzmiAinda não há avaliações
- Introduction To Fixed Pertial Dentures (GTC)Documento5 páginasIntroduction To Fixed Pertial Dentures (GTC)Thesdave SinghAinda não há avaliações
- Relining and Rebasing of Complete DentureDocumento7 páginasRelining and Rebasing of Complete DentureAdinda YokoAinda não há avaliações
- Space MaintainerDocumento2 páginasSpace MaintainerFibrianti SeputriAinda não há avaliações
- Final PDLDocumento100 páginasFinal PDLDrRahat SaleemAinda não há avaliações
- Failures of Restorations / Orthodontic Courses by Indian Dental AcademyDocumento44 páginasFailures of Restorations / Orthodontic Courses by Indian Dental Academyindian dental academyAinda não há avaliações
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDocumento6 páginasEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargAinda não há avaliações
- Diagnosis and Diagnostic Adis in Endodontics - Copy (100668749)Documento39 páginasDiagnosis and Diagnostic Adis in Endodontics - Copy (100668749)kapilphysio100% (1)
- PulpDocumento54 páginasPulpAnsh DuttaAinda não há avaliações
- Dental IndicesDocumento71 páginasDental IndicesTin Maw100% (4)
- Denture CleansearDocumento41 páginasDenture CleanseardrsaruAinda não há avaliações
- Tooth Carving Exercise As A Foundation For Future Dental Career - A ReviewDocumento3 páginasTooth Carving Exercise As A Foundation For Future Dental Career - A ReviewRik ChatterjeeAinda não há avaliações
- Design of A Removable Partial Denture: by Taseef Hasan Farook, BDS (Final Year, University of Dhaka)Documento70 páginasDesign of A Removable Partial Denture: by Taseef Hasan Farook, BDS (Final Year, University of Dhaka)Novita RAinda não há avaliações
- Clinical Portfolio EndoDocumento16 páginasClinical Portfolio EndodrhijaziAinda não há avaliações
- Oral Surgery Volume 4, Extraction and Impacted TeethDocumento32 páginasOral Surgery Volume 4, Extraction and Impacted TeethskyangkorAinda não há avaliações
- Mechanical Plaque ControlDocumento58 páginasMechanical Plaque ControlNeelam Khalia100% (1)
- Post and Core Orthodontic Courses by Indian Dental AcademyDocumento46 páginasPost and Core Orthodontic Courses by Indian Dental AcademyPadmini Reddy100% (1)
- Extrac 1Documento49 páginasExtrac 1api-19916399Ainda não há avaliações
- Tooth SeparationDocumento26 páginasTooth SeparationPriyal KhandelwalAinda não há avaliações
- Conservative DentistryDocumento6 páginasConservative DentistryAbdallah Essam Al-ZireeniAinda não há avaliações
- Developmental Disturbances of TeethDocumento65 páginasDevelopmental Disturbances of Teethisraa0dentist100% (4)
- Post and CoreDocumento26 páginasPost and CoreIbrahim Elnaggar0% (1)
- Tooth Eruption and SheddingDocumento29 páginasTooth Eruption and Sheddingjenny girl100% (1)
- Modern Anterior Endodontic Access and Directed Dentin Conservation David Clark & John Khademi PDFDocumento5 páginasModern Anterior Endodontic Access and Directed Dentin Conservation David Clark & John Khademi PDFizeldien5870Ainda não há avaliações
- Development of OcclusionDocumento9 páginasDevelopment of OcclusionЕленаAinda não há avaliações
- Introduction To Composite RestorationsDocumento28 páginasIntroduction To Composite RestorationsAhmad Fawzi100% (2)
- Role of Neutrophils in Periodontal DiseaseDocumento65 páginasRole of Neutrophils in Periodontal DiseaseGaurav Phaphriya40% (5)
- Ultrastructure and Functions of CementumDocumento106 páginasUltrastructure and Functions of CementumJaya Shakthi0% (1)
- Complicated ExodontiaDocumento41 páginasComplicated Exodontiamiss0meAinda não há avaliações
- Canine Impaction Oral SurgeryDocumento6 páginasCanine Impaction Oral SurgeryFourthMolar.comAinda não há avaliações
- Success& Failures in EndoDocumento32 páginasSuccess& Failures in Endorasagna reddyAinda não há avaliações
- Conservative Dentistry and Endodontics Question PaperDocumento37 páginasConservative Dentistry and Endodontics Question PapersamhitaAinda não há avaliações
- Comparison of One Versus Multi Visit Tic TreatmentDocumento47 páginasComparison of One Versus Multi Visit Tic TreatmentamitdrsAinda não há avaliações
- Recent Advances in DentistryDocumento2 páginasRecent Advances in DentistrySudarsan SangeethaAinda não há avaliações
- Panoramic RadiographyDocumento31 páginasPanoramic RadiographyMohammed abdalmenem100% (1)
- Seminar 6 Preventive Prosthodontics in CD WordDocumento29 páginasSeminar 6 Preventive Prosthodontics in CD Wordketaki kunteAinda não há avaliações
- Imaging in Periodontics PerioDocumento49 páginasImaging in Periodontics PerioFourthMolar.comAinda não há avaliações
- Dental Implant Course in ChennaiDocumento2 páginasDental Implant Course in ChennaiRishabh Madhu SharanAinda não há avaliações
- Bal Satyarth PrakashDocumento6 páginasBal Satyarth PrakashRishabh Madhu SharanAinda não há avaliações
- AppoloDocumento2 páginasAppoloRishabh Madhu SharanAinda não há avaliações
- Get Ready To Witness The Cracking Cricketing Action!!: Inter House Cricket ChampionshipDocumento1 páginaGet Ready To Witness The Cracking Cricketing Action!!: Inter House Cricket ChampionshipRishabh Madhu SharanAinda não há avaliações
- 8 Tips For Teachers: Needed Accommodations in The Classroom. Respect The Student's Needs, ButDocumento6 páginas8 Tips For Teachers: Needed Accommodations in The Classroom. Respect The Student's Needs, ButRishabh Madhu SharanAinda não há avaliações
- Bal Satyarth PrakashDocumento97 páginasBal Satyarth PrakashSubramanya PaiAinda não há avaliações
- Physics Rotational Motion MCQDocumento7 páginasPhysics Rotational Motion MCQrkjha70867% (3)
- Number SystemsDocumento47 páginasNumber SystemsRishabh Madhu SharanAinda não há avaliações
- A Very Warm Good Evening To All The Wonderful People Present HereDocumento10 páginasA Very Warm Good Evening To All The Wonderful People Present HereRishabh Madhu SharanAinda não há avaliações
- Principle of PanormicDocumento64 páginasPrinciple of PanormicRishabh Madhu Sharan100% (1)
- Pola Winning Flyer en A4Documento1 páginaPola Winning Flyer en A4Rishabh Madhu SharanAinda não há avaliações
- Rotary Cutting Instruments1Documento30 páginasRotary Cutting Instruments1Rishabh Madhu SharanAinda não há avaliações
- Splinting Teeth - A Review of Methodology and Clinical Case ReportsDocumento4 páginasSplinting Teeth - A Review of Methodology and Clinical Case ReportsRishabh Madhu SharanAinda não há avaliações
- Applications in Dermatology, Dentistry and Lasik Eye Surgery Using LasersDocumento10 páginasApplications in Dermatology, Dentistry and Lasik Eye Surgery Using LasersRishabh Madhu SharanAinda não há avaliações
- Welcome SpeechDocumento3 páginasWelcome SpeechRishabh Madhu SharanAinda não há avaliações
- Types of Maxillofacial ProsthesisDocumento65 páginasTypes of Maxillofacial ProsthesisRishabh Madhu Sharan100% (2)
- Anti-Plaque & Anti-Calculus AgentsDocumento43 páginasAnti-Plaque & Anti-Calculus AgentsRishabh Madhu SharanAinda não há avaliações
- Appearance of Anatomic Structures On Panoramic ImageDocumento18 páginasAppearance of Anatomic Structures On Panoramic ImageRishabh Madhu SharanAinda não há avaliações
- History Paper 2 IB Study GuideDocumento6 páginasHistory Paper 2 IB Study Guidersuresh1995100% (4)
- RARC Letter To Tan Seri Razali Ismail July 26-2013Documento4 páginasRARC Letter To Tan Seri Razali Ismail July 26-2013Rohingya VisionAinda não há avaliações
- Persona Core Poster - Creative Companion1 PDFDocumento1 páginaPersona Core Poster - Creative Companion1 PDFAdemola OgunlaluAinda não há avaliações
- Conducting A SeminarDocumento17 páginasConducting A SeminarSubhash DhungelAinda não há avaliações
- Design & Evaluation in The Real World: Communicators & Advisory SystemsDocumento13 páginasDesign & Evaluation in The Real World: Communicators & Advisory Systemsdivya kalyaniAinda não há avaliações
- Oscar Characterization TemplateDocumento3 páginasOscar Characterization Templatemqs786Ainda não há avaliações
- Cheat SheetDocumento2 páginasCheat SheetFrancis TanAinda não há avaliações
- Ocr Graphics Gcse CourseworkDocumento6 páginasOcr Graphics Gcse Courseworkzys0vemap0m3100% (2)
- Servicenow Rest Cheat SheetDocumento3 páginasServicenow Rest Cheat SheetHugh SmithAinda não há avaliações
- Kepimpinan BerwawasanDocumento18 páginasKepimpinan BerwawasanandrewanumAinda não há avaliações
- Jataka Tales - The Crane and The CrabDocumento5 páginasJataka Tales - The Crane and The Crabshahrajan2k1Ainda não há avaliações
- Thai Reader Project Volume 2Documento215 páginasThai Reader Project Volume 2geoffroAinda não há avaliações
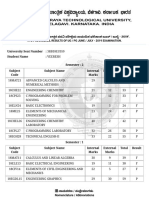
- VTU Result PDFDocumento2 páginasVTU Result PDFVaibhavAinda não há avaliações
- Evaluation of The Performance of HRCT in The Diagnostic and Management of Covid-19Documento7 páginasEvaluation of The Performance of HRCT in The Diagnostic and Management of Covid-19IJAR JOURNALAinda não há avaliações
- U6 - S7 - Trabajo Individual 7 - Ficha de Aplicación INGLES 3Documento2 páginasU6 - S7 - Trabajo Individual 7 - Ficha de Aplicación INGLES 3Antonio Andres Duffoo MarroquinAinda não há avaliações
- Sindhudurg Kokan All Tourism Spot Information WWW - Marathimann.inDocumento54 páginasSindhudurg Kokan All Tourism Spot Information WWW - Marathimann.inMarathi Mann92% (12)
- Computer Literacy Skills and Self-Efficacy Among Grade-12 - Computer System Servicing (CSS) StudentsDocumento25 páginasComputer Literacy Skills and Self-Efficacy Among Grade-12 - Computer System Servicing (CSS) StudentsNiwre Gumangan AguiwasAinda não há avaliações
- Ant Colony AlgorithmDocumento11 páginasAnt Colony Algorithmjaved765Ainda não há avaliações
- Impact of E-Banking in India: Presented By-Shouvik Maji PGDM - 75Documento11 páginasImpact of E-Banking in India: Presented By-Shouvik Maji PGDM - 75Nilanjan GhoshAinda não há avaliações
- Blue Mountain Coffee Case (ADBUDG)Documento16 páginasBlue Mountain Coffee Case (ADBUDG)Nuria Sánchez Celemín100% (1)
- Deception With GraphsDocumento7 páginasDeception With GraphsTanmay MaityAinda não há avaliações
- A Complete List of Greek Underworld GodsDocumento3 páginasA Complete List of Greek Underworld GodsTimothy James M. Madrid100% (1)
- Social Contract Theory - Internet Encyclopedia of PhilosophyDocumento28 páginasSocial Contract Theory - Internet Encyclopedia of Philosophywolf1804100% (1)
- Imam Muhammad Baqir (As) BioDocumento5 páginasImam Muhammad Baqir (As) BioFatema AbbasAinda não há avaliações
- Hinog vs. MellicorDocumento11 páginasHinog vs. MellicorGreta VilarAinda não há avaliações
- Indicator For Meridian Diagnosis AGNIS BAT 02 (User's Manual) AGNISDocumento5 páginasIndicator For Meridian Diagnosis AGNIS BAT 02 (User's Manual) AGNISssmaddiAinda não há avaliações
- K 46 Compact Spinning Machine Brochure 2530-V3 75220 Original English 75220Documento28 páginasK 46 Compact Spinning Machine Brochure 2530-V3 75220 Original English 75220Pradeep JainAinda não há avaliações
- OITE - MCQ S QuestionsFinal2011Documento67 páginasOITE - MCQ S QuestionsFinal2011KatKut99100% (7)
- Basic Trigonometric FunctionDocumento34 páginasBasic Trigonometric FunctionLony PatalAinda não há avaliações
- 208 C - Algebras: Marc Rieffel Notes by Qiaochu Yuan Spring 2013Documento55 páginas208 C - Algebras: Marc Rieffel Notes by Qiaochu Yuan Spring 2013Nikos AthanasiouAinda não há avaliações
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Nota: 3 de 5 estrelas3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNo EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDNota: 5 de 5 estrelas5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityNo EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityNota: 4 de 5 estrelas4/5 (29)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNo EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionNota: 4 de 5 estrelas4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsAinda não há avaliações
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedNota: 5 de 5 estrelas5/5 (81)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNota: 2 de 5 estrelas2/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNo EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessNota: 4.5 de 5 estrelas4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossNo EverandThe Obesity Code: Unlocking the Secrets of Weight LossNota: 4 de 5 estrelas4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNo EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaNota: 4.5 de 5 estrelas4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNo EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisNota: 4.5 de 5 estrelas4.5/5 (42)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNo EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsNota: 4 de 5 estrelas4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNota: 5 de 5 estrelas5/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNo EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeNota: 4.5 de 5 estrelas4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.No EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Nota: 4.5 de 5 estrelas4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityNo EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityNota: 4 de 5 estrelas4/5 (5)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNo EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisNota: 4 de 5 estrelas4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNo EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryNota: 4 de 5 estrelas4/5 (45)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNo EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsNota: 4.5 de 5 estrelas4.5/5 (170)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNo EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedNota: 4 de 5 estrelas4/5 (61)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNo EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesNota: 4.5 de 5 estrelas4.5/5 (1412)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNo EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNota: 1 de 5 estrelas1/5 (1)
- The Marshmallow Test: Mastering Self-ControlNo EverandThe Marshmallow Test: Mastering Self-ControlNota: 4.5 de 5 estrelas4.5/5 (59)