Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Double Lumen Catheter Dr. Ahmad GhozaliDocumento20 páginasDouble Lumen Catheter Dr. Ahmad GhozaliastarimediantoAinda não há avaliações
- Anesthesia MachineDocumento17 páginasAnesthesia Machineتبارك موسى كريم علوان0% (1)
- Appendectomy/ Appendicitis Case StudyDocumento15 páginasAppendectomy/ Appendicitis Case StudyApril93% (30)
- Lecture 20 CarcinogenesisDocumento84 páginasLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- The BreastDocumento72 páginasThe BreastMohammad_Islam87Ainda não há avaliações
- Physiopathology SyllabusDocumento1 páginaPhysiopathology SyllabusMohammad_Islam87Ainda não há avaliações
- Lecture 17 DiabetesDocumento51 páginasLecture 17 DiabetesMohammad_Islam87Ainda não há avaliações
- Lecture 18 Upper Digestive DiseasesDocumento63 páginasLecture 18 Upper Digestive DiseasesMohammad_Islam87Ainda não há avaliações
- The LymphomasDocumento46 páginasThe LymphomasMohammad_Islam87Ainda não há avaliações
- Pharmacology Lecture 12-5-2009, OpiodsDocumento18 páginasPharmacology Lecture 12-5-2009, OpiodsMohammad_Islam87Ainda não há avaliações
- Curst Um Abd EnglDocumento10 páginasCurst Um Abd EnglMohammad_Islam87Ainda não há avaliações
- Abdominal HerniaeDocumento66 páginasAbdominal HerniaeMohammad_Islam87Ainda não há avaliações
- Plastic SurgeryDocumento11 páginasPlastic SurgeryMohammad_Islam87Ainda não há avaliações
- Liver Curs 2009Documento215 páginasLiver Curs 2009Mohammad_Islam87Ainda não há avaliações
- ?#ry%oefr: - J4 @,8/ MryDocumento15 páginas?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Ainda não há avaliações
- AnaemiaDocumento83 páginasAnaemiaMohammad_Islam87100% (2)
- Pharmacology Lecture 19-5-2009, NSAIDSDocumento19 páginasPharmacology Lecture 19-5-2009, NSAIDSMohammad_Islam87Ainda não há avaliações
- Borcane TumorDocumento14 páginasBorcane TumorMohammad_Islam87Ainda não há avaliações
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDocumento25 páginasMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Ainda não há avaliações
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDocumento29 páginasMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Ainda não há avaliações
- Morphopathology Macroscopy (Romanian-Batch)Documento187 páginasMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDocumento19 páginasMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Ainda não há avaliações
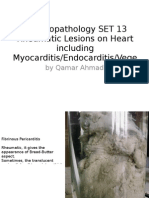
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDocumento25 páginasMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Ainda não há avaliações
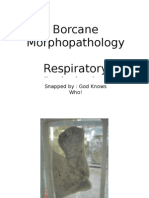
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento11 páginasBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Ainda não há avaliações
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento7 páginasBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Pharmacology Lecture Diuretic Agents (High Quality)Documento15 páginasPharmacology Lecture Diuretic Agents (High Quality)Mohammad_Islam87Ainda não há avaliações
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDocumento18 páginasMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Ainda não há avaliações
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento7 páginasBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Ainda não há avaliações
- Workshop 20Documento2 páginasWorkshop 20Mohammad_Islam87Ainda não há avaliações
- Pharmacology Lecture 5-5-2009Documento15 páginasPharmacology Lecture 5-5-2009Mohammad_Islam87Ainda não há avaliações
- Conditions Presenting With Abdominal PainDocumento69 páginasConditions Presenting With Abdominal PainaimanAinda não há avaliações
- Workshop 19Documento3 páginasWorkshop 19Mohammad_Islam87Ainda não há avaliações
- Engl BUN - EditDocumento167 páginasEngl BUN - EditMohammad_Islam87Ainda não há avaliações
- State Consumer Disputes Redressal Commission, Punjab, ChandigarhDocumento50 páginasState Consumer Disputes Redressal Commission, Punjab, ChandigarhKandlagunta Gayathri PraharshithaAinda não há avaliações
- Chapt 1 PeterDocumento63 páginasChapt 1 PeterSamson PeterAinda não há avaliações
- Orthopedic Outcomes of Hybrid and Conventional Hyrax Expanders Par Daniela Garib Angle Ortho 2021Documento9 páginasOrthopedic Outcomes of Hybrid and Conventional Hyrax Expanders Par Daniela Garib Angle Ortho 2021NANA NANA Arnel redonAinda não há avaliações
- UNEP Directory March 2021Documento23 páginasUNEP Directory March 2021Chris JohnAinda não há avaliações
- I. Attention Getter: in Today's Society, There Is: A. Overview: Most People Don't Know WhoDocumento5 páginasI. Attention Getter: in Today's Society, There Is: A. Overview: Most People Don't Know WhoalexAinda não há avaliações
- Inguinal Hernias in Adults Epidemiological Clinical and Therapeutic AspectsDocumento24 páginasInguinal Hernias in Adults Epidemiological Clinical and Therapeutic AspectsmutmainnahAinda não há avaliações
- TAOMS20 Abstract BookDocumento238 páginasTAOMS20 Abstract BookTaha ÖzerAinda não há avaliações
- Biografija: DR - Sc. Mirza MoranjkićDocumento2 páginasBiografija: DR - Sc. Mirza MoranjkićEnis HuskanovicAinda não há avaliações
- Reprentation-Dr Jamshaid Rahim Shaikh Zaid HospitalDocumento5 páginasReprentation-Dr Jamshaid Rahim Shaikh Zaid HospitalGM UDAinda não há avaliações
- Shoulder Arthroscopy, Anatomy and Variants - Part 1Documento6 páginasShoulder Arthroscopy, Anatomy and Variants - Part 1Raluca CostandacheAinda não há avaliações
- CPC 0 Series QuestionsDocumento6 páginasCPC 0 Series Questions19ucs175Ainda não há avaliações
- 2002 Vol.40 Issues 4 Vascular Imaging PDFDocumento278 páginas2002 Vol.40 Issues 4 Vascular Imaging PDFRivani KurniawanAinda não há avaliações
- Sexual Medicine ReviewsDocumento14 páginasSexual Medicine ReviewsilhamAinda não há avaliações
- Carotid Blowout PDFDocumento2 páginasCarotid Blowout PDFBkas GrgAinda não há avaliações
- Closure of Oroantral Communications A Review of The LiteratureDocumento8 páginasClosure of Oroantral Communications A Review of The LiteratureFaisal H RanaAinda não há avaliações
- Complex Head and Neck Microvascular - SurgeryDocumento327 páginasComplex Head and Neck Microvascular - Surgerydoctorsoha.shAinda não há avaliações
- Medical-Surgical Nursing 1: Pamantasan NG Lungsod NG MaynilaDocumento3 páginasMedical-Surgical Nursing 1: Pamantasan NG Lungsod NG MaynilaAye DumpAinda não há avaliações
- Womac Hip Score (WHS) : Pain Severity (On Average) During The Past MonthDocumento3 páginasWomac Hip Score (WHS) : Pain Severity (On Average) During The Past MonthPetru CarajaAinda não há avaliações
- Text Book of Ocular Pharmacology and Therapeutics: Ram Lal SharmaDocumento2 páginasText Book of Ocular Pharmacology and Therapeutics: Ram Lal SharmaMudassar SattarAinda não há avaliações
- Coagulation Support During Perioperative Bleeding ManagementDocumento4 páginasCoagulation Support During Perioperative Bleeding ManagementAndrew MihaiAinda não há avaliações
- Association Between Frailty and Time Alive and at Home After Cancer Surgery Among Older Adults: A Population-Based AnalysisDocumento19 páginasAssociation Between Frailty and Time Alive and at Home After Cancer Surgery Among Older Adults: A Population-Based AnalysisJuan Camilo SánchezAinda não há avaliações
- Atoz Orthodontics: Rthodontic MCQDocumento112 páginasAtoz Orthodontics: Rthodontic MCQAbdo SerboutiAinda não há avaliações
- The Millennium: Core MessagesDocumento8 páginasThe Millennium: Core MessagesCharbel TadrosAinda não há avaliações
- Periimplant Soft Tissue Management in Patients With A Fibula Free Flap Reconstruction Case Series and Description of A New TechniqueDocumento6 páginasPeriimplant Soft Tissue Management in Patients With A Fibula Free Flap Reconstruction Case Series and Description of A New TechniqueSudheer KondakaAinda não há avaliações
- 2023 JBJS Reviews Clavicular Fractures in The AsolescentDocumento10 páginas2023 JBJS Reviews Clavicular Fractures in The AsolescentjcmarecauxlAinda não há avaliações
- Okuno 2014Documento4 páginasOkuno 2014mujtabaAinda não há avaliações
- Operative Techniques in General Surgery: Kevin E. BehrnsDocumento1 páginaOperative Techniques in General Surgery: Kevin E. BehrnsAndres BernalAinda não há avaliações