Você também pode gostar
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- PE11 Q4 Module4a Weeks1and2Documento19 páginasPE11 Q4 Module4a Weeks1and2Rizza Mhae Rebanal75% (8)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
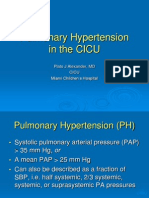
- Pulmonary Hypertension in The CICUDocumento50 páginasPulmonary Hypertension in The CICUCardiacCareCenterMCHAinda não há avaliações
- Case Study EssayDocumento19 páginasCase Study EssaylecharmedenuitAinda não há avaliações
- Immunology: 'S CompanionsDocumento74 páginasImmunology: 'S CompanionsRoahit RajanAinda não há avaliações
- Cancer Program SeminarDocumento98 páginasCancer Program SeminarhemihemaAinda não há avaliações
- HLHS and SVDocumento66 páginasHLHS and SVCardiacCareCenterMCHAinda não há avaliações
- Arterial Switch OperationDocumento15 páginasArterial Switch OperationCardiacCareCenterMCH100% (1)
- Post-Pericardiotomy Syndrome - May 22Documento18 páginasPost-Pericardiotomy Syndrome - May 22CardiacCareCenterMCHAinda não há avaliações
- Jane Salvaggio ARNP CV SurgeryDocumento23 páginasJane Salvaggio ARNP CV SurgeryCardiacCareCenterMCHAinda não há avaliações
- The Use of Svo2 Monitoring in The Cardiac Intensive Care UnitDocumento60 páginasThe Use of Svo2 Monitoring in The Cardiac Intensive Care UnitAnthony RossiAinda não há avaliações
- Alcapa FinalDocumento22 páginasAlcapa FinalCardiacCareCenterMCHAinda não há avaliações
- Overview OfCongenitalCardiacDiseaseDocumento98 páginasOverview OfCongenitalCardiacDiseaseCardiacCareCenterMCHAinda não há avaliações
- From TOF To PA Nurses - FinalDocumento44 páginasFrom TOF To PA Nurses - FinalCardiacCareCenterMCH100% (1)
- Pediatric Airway ManagementDocumento54 páginasPediatric Airway ManagementCardiacCareCenterMCHAinda não há avaliações
- Cardiac Arrhythmia EmergenciesDocumento65 páginasCardiac Arrhythmia EmergenciesCardiacCareCenterMCHAinda não há avaliações
- Jadwal PM Igd 2023Documento48 páginasJadwal PM Igd 2023Sugeng NugrohoAinda não há avaliações
- Limfoproliferari Cronice MaligneDocumento18 páginasLimfoproliferari Cronice MaligneAlice MuscaAinda não há avaliações
- BupropionDocumento3 páginasBupropionRJ HAinda não há avaliações
- Prepsheet Study Guide Med AdminDocumento7 páginasPrepsheet Study Guide Med AdminHannaAinda não há avaliações
- Adobe Scan Nov 27, 2022Documento3 páginasAdobe Scan Nov 27, 2022Wilson PintoAinda não há avaliações
- Diabetes Advisor - A Medical Expert System For Diabetes ManagementDocumento5 páginasDiabetes Advisor - A Medical Expert System For Diabetes ManagementPrincess LunieAinda não há avaliações
- Ake Quick Action If Someone Is Choking On A Swallowed ObjectDocumento29 páginasAke Quick Action If Someone Is Choking On A Swallowed ObjectYAMINIPRIYANAinda não há avaliações
- Baxter Revaclear - Datasheet - 2020 - A4 - GBU-RC38-200001 - Low - 0Documento2 páginasBaxter Revaclear - Datasheet - 2020 - A4 - GBU-RC38-200001 - Low - 0Black MonkeyAinda não há avaliações
- References WBCDocumento2 páginasReferences WBCMiguelito Galagar GultianoAinda não há avaliações
- Cardiogeneicpulmonaryedema December2019Documento9 páginasCardiogeneicpulmonaryedema December2019Amaranto Santoso ongkoAinda não há avaliações
- Pre Op GuidelinesDocumento11 páginasPre Op GuidelinesHanif FebrianAinda não há avaliações
- Psychological Aspects of Living With HIV Disease: PracticeDocumento4 páginasPsychological Aspects of Living With HIV Disease: PracticeAntro BerrinAinda não há avaliações
- Food AllergyDocumento2 páginasFood Allergydyfc25Ainda não há avaliações
- Chapter 5 DRUG EDUCDocumento38 páginasChapter 5 DRUG EDUCRiza Roxanne ManongdoAinda não há avaliações
- Annex 8. Viral Transport Media (VTM)Documento2 páginasAnnex 8. Viral Transport Media (VTM)deancoksAinda não há avaliações
- New Patient Needing Continuous Renal Replacement Therapy (CRRT)Documento9 páginasNew Patient Needing Continuous Renal Replacement Therapy (CRRT)sergey_1972Ainda não há avaliações
- Manejo de Conducta en Niños Ansiosos. (ING)Documento6 páginasManejo de Conducta en Niños Ansiosos. (ING)Ale RamírezAinda não há avaliações
- SimvastatinDocumento1 páginaSimvastatinLyka Mae Imbat - PacnisAinda não há avaliações
- 4 - Nephritic SyndromeDocumento2 páginas4 - Nephritic SyndromeDrhisham AttiaAinda não há avaliações
- Transverse MyelitisDocumento7 páginasTransverse MyelitisAmr BashaAinda não há avaliações
- Hyperemesis GravidarumDocumento7 páginasHyperemesis GravidarumPrawira Weka AkbariAinda não há avaliações
- WJCCM 11 33Documento8 páginasWJCCM 11 33medicshinobiAinda não há avaliações
- Anatomic and Visual Function Outcomes in Paediatric Idiopathic Intracranial HypertensionDocumento6 páginasAnatomic and Visual Function Outcomes in Paediatric Idiopathic Intracranial HypertensionRani PittaAinda não há avaliações
- High Dose Rate Interstitial Brachytherapy Using Two Weekly SessionsDocumento1 páginaHigh Dose Rate Interstitial Brachytherapy Using Two Weekly SessionsZuriAinda não há avaliações
- Specialize Immunity at Epithelial Barriers and in Immune Privilege TissuesDocumento27 páginasSpecialize Immunity at Epithelial Barriers and in Immune Privilege TissuesUmar UsmanAinda não há avaliações
- Psychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice Townsend 7th Edition Test BankDocumento24 páginasPsychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice Townsend 7th Edition Test BankAnitaCareyfemy100% (35)